

Updated terminology for gamete and embryo donors: directed (identified) to replace ‘‘known’’ and nonidentified to replace ‘‘anonymous’’: a committee opinion
Download a PDF of this documentSocial media, changing mores, and more recently significantly broader access to direct-to-consumer deoxyribonucleic acid (DNA) testing (DTC DNA) have all contributed to a new reality that expectations of donor anonymity can no longer be assured. It is estimated that at the present time, tens of millions of Americans have their genetic information stored in privately owned and largely unregulated databases (1).
Other modalities such as facial recognition have also recently become refined and more accurate (2). These technologies have introduced a means by which donor-conceived offspring and those to whom they have genetic ties may identify, locate, and contact one another. It should be noted that individuals who donated gametes or embryos, or who are donor conceived, may be traceable even if they never enroll in any DNA testing program themselves. This may occur if others with genetic ties to them participate in DTC DNA programs that allow for the identification of those to whom they are genetically linked (3). The era of perpetual donor anonymity has ended. This loss of anonymity has the potential to affect both current and past donations, including donors, recipients, donor-conceived offspring, and those who are genetically linked to them. While donor identity can still be withheld at the time of a donation, the discovery of genetic relationships leading to gamete and embryo donor identification may occur both outside the control of medical professionals and indefinitely into the future.
These emerging genetic and technological realities have changed the landscape of gamete and embryo donation, necessitating a concomitant change in the language used to describe these donations and in the counseling of those who participate in them.
As such, the American Society for Reproductive Medicine has changed the nomenclature of gamete and embryo donation. Donors who were previously described as known will now be referred to as directed (identified) donors, and those previously described as anonymous will be referred to as non- identified donors.
DIRECTED DONORS
The choice of the term directed (identified) donor, previously called known donor, was selected to align with the Food and Drug Administration (FDA) regulations (4). The gametes from a directed (identified) donor who is deemed ‘‘ineligible’’ based on FDA guidance for tissue donation may in some cases be used if both parties are aware of the theoretical infectious or genetic risks to the recipient(s) and offspring and consent to move forward with the donation (5). The categorization of an individual as a directed (identified) donor affords recipients the option of waiving some exclusion criteria when they value the benefits of the known donor (e.g., sister to sister egg donation) so strongly that they are willing to accept the presumably low risk of infectious disease transmission. The use of the term directed (identified) mirrors the FDA language that specifies exclusions and exceptions for gamete and embryo donation based on whether the parties are known to one another. The new terminology should assist physicians and administrators as they interpret and apply the FDA regulations to clinical practice.NONIDENTIFIED DONORS
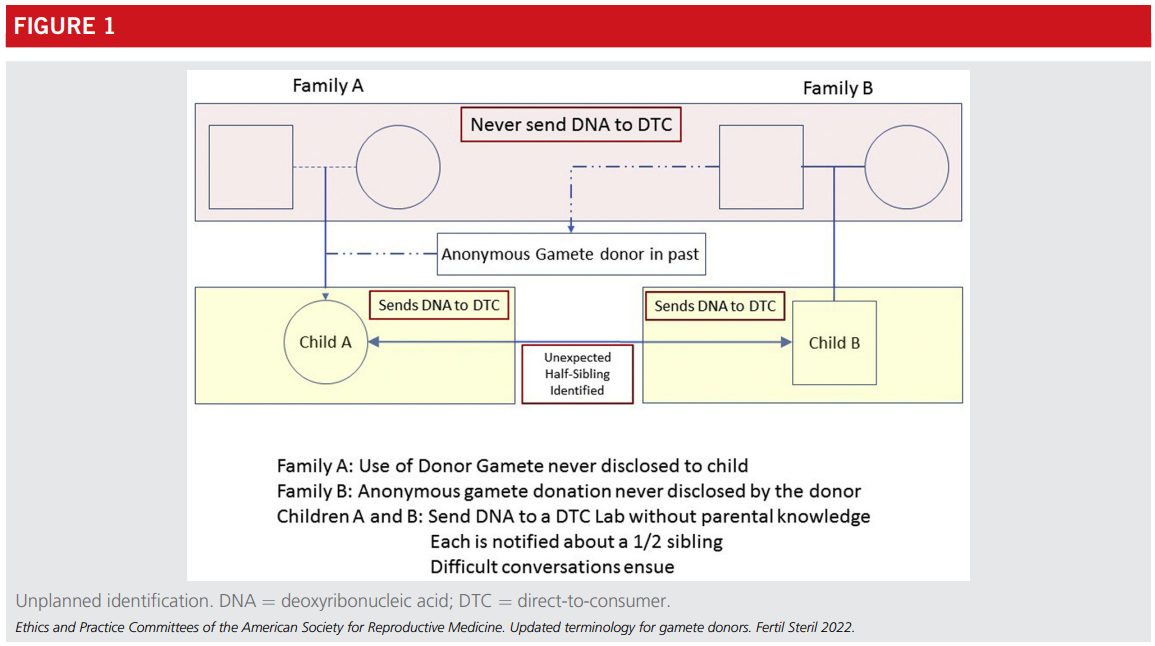
The choice of the term nonidentified for those who were previously called anonymous donors acknowledges the intention of all involved in the donation process, including donors and recipients, as well as any medical, professional, or coordinating entities or professionals, not to share identifying information of the donor or recipient with one another. The intention at the time a nonidentified donation contract is entered into, or the donation undertaken, is that the identities of the donor, recipient, and any resulting offspring will remain unknown to one another to the extent permitted under law or to an explicit and limited degree, such as when a contract or consent document may allow for arranging contact between the donor-conceived offspring and the donor upon the offspring reaching a specific age, often the age of majority. These latter types of arrangements are sometimes referred to as open-identity arrangements, and the donors who agree to them are referred to as open-identity donors.Example of unplanned identification (Figure 1): Family A: Use of donor gamete never disclosed to child. Family B: ‘‘Anonymous’’ gamete donation never disclosed by the donor. Children A and B: Independently send DNA to a DTC DNA Laboratory without parental knowledge. Each is notified about a 1/2 sibling. Difficult conversations ensue.
CONCLUSION
In conclusion, given a multitude of global social media platforms, increasingly accessible and used DTC DNA services, and facial recognition technology, true anonymity between donors and recipients can no longer be guaranteed. All parties involved in gamete and embryo donation should be aware that identities may be discovered by the resulting offspring and other genetically linked individuals at any future time. This holds for both directed (identified) and nonidentified do- nations. Complicating matters is the fact that past donors, whether they donated with the intention of anonymity or not, are now potentially discoverable at any future date. The extent to which such revelations will occur is unknown. A 2019 estimate suggested that approximately 8% of the US population had already sent DNA to a DTC DNA vendor with speculation that the number could more than triple over the next several years, thus greatly expanding the population of people who can identify one another based on their genetic links (6). A related, but somewhat different, scenario is the active pursuit of connection among offspring who know they were conceived from donor gametes or embryos (7).The impact that this will have on those being discovered and whether this current reality will change the willingness of individuals to serve as gamete or embryo donors remain to be seen. The collateral effects on genetically linked individuals much removed from the donation process are also unknown but will become clearer over time. Critical to the donation process is the informed consent of donors and recipients regarding the possibility that genetically linked individuals may identify one another, both intentionally and otherwise, at any future date.
Physicians and those who arrange gamete and embryo donation should provide maximum transparency regarding the limits of anonymity to all known stakeholders at the time of the donation, beginning with the change in nomenclature when referring to directed (identified) and nonidentified gamete and embryo donors.
Acknowledgments: This report was developed under the direction of the Practice and Ethics Committees of the American Society for Reproductive Medicine (ASRM) as a service to its members and other practicing clinicians. Although this document reflects appropriate management of a problem encountered in the practice of reproductive medicine, it is not intended to be the only approved standard of practice or dictate an exclusive course of treatment. Other plans of management may be appropriate, taking into account the needs of the individual patient, available resources, and institutional or clinical practice limitations. The Practice and Ethics Committees and the Board of Directors of the American Society for Reproductive Medicine have approved this report.
This document was reviewed by the ASRM members, and their input was considered in the preparation of the final document. The following members of the ASRM Practice and Ethics Committees participated in the development of this document: Alan Penzias, MD; Kristin Bendikson, MD; Marcelle I. Cedars, MD; Tommaso Falcone, MD; Karl Hansen, MD, PhD; Micah Hill, DO; Sangita Jindal, PhD; Suleena Kalra, MD, MSCE; Jennifer Mersereau, MD; Catherine Racowsky, PhD; Richard Reindollar, MD; Chevis N Shannon, DrPH, MPH, MBA; Anne Steiner, MD, MPH; Cigdem Tanrikut, MD; Michael Thomas, MD; Belinda Yauger, MD; Sigal Klipstein, MD; Deborah Anderson; Kavita Shah Arora, MD, MBE; Tolulope Bakare, MD; Katherine Cameron, MD; Susan Crockin, JD; Ruth Farrell, MD; Catherine Hammack-Aviran, MA, JD; Mandy Katz-Jaffe, PhD; Jennifer Kawwass, MD; Ed- ward Martinez, MD; Joshua Morris, MD; Robert Rebar, MD; Eli Reshef, MD; Chevis N Shannon, DrPH, MPH, MBA; Hugh Taylor, MD; Sean Tipton, MA; and Julianne Zweifel, PhD. All Committee members disclosed commercial and financial relationships with manufacturers or distributors of goods or services used to treat patients. The members of the Committees who were found to have conflicts of interest based on the relationships disclosed did not participate in the discussion or development of this document.
REFERENCES
- Regalado A. 2017 was the year consumer DNA testing blew up. Available at: https://www.technologyreview.com/2018/02/12/145676/2017-was-the-year- consumer-dna-testing-blew-up/. Accessed March 23, 2022.
- Harwell D. This facial recognition website can turn anyone into a cop—or a stalker. Available at: https://www.washingtonpost.com/technology/2021/ 05/14/pimeyes-facial-recognition-search-secrecy. Accessed March 23, 2022.
- 23andMe Customer Care. What unexpected things might I learn from 23andMe?. Available at: https://customercare.23andme.com/hc/en-us/ articles/202907980. Accessed March 23, 2022.
- US Food and Drug Administration. Eligibility determination for donors of human cells, tissues, and cellular and tissue-based products: guidance for industry. Available at: https://www.fda.gov/regulatory-information/search-fda-guidance- documents/eligibility-determination-donors-human-cells-tissues-and- cellular-and-tissue-based-products. Accessed March 23, 2022.
- Practice Committee of the American Society for Reproductive Medicine, Practice Committee for the Society for Assisted Reproductive Technology. Guidance regarding gamete and embryo donation. Fertil Steril 2021;115:1395–410.
- Regalado A. More than 26 million people have taken an at-home ancestry test. Available at: https://www.technologyreview.com/2019/02/11/103446/ more-than-26-million-people-have-taken-an-at-home-ancestry-test. Ac- cessed March 23, 2022.
- Dominus S. Sperm donors can’t stay secret any more. Here’s what that means. Available at: https://www.nytimes.com/2019/06/26/magazine/sperm-donor- questions.html. Accessed March 23, 2022.
Ethics Opinions
Ethical considerations of in vitro gametogenesis: an Ethics Committee opinion ASRM (2026)
In vitro gametogenesis (IVG) represents a potentially transformative yet currently experimental frontier in reproductive science.
Compassionate transfer: patient requests for embryo transfer for nonreproductive purposes (2026)
A patient request to transfer embryos into her body in a location or at a time when pregnancy is highly unlikely ...
Fertility preservation and reproduction in patients facing gonadotoxic therapies or gonadectomy: an Ethics Committee opinion (2026)
Patients receiving gonadotoxic treatment should be informed of options for fertility preservation and future reproduction prior to such treatment.
Use of preimplantation genetic testing for polygenic disorders (PGT-P): an Ethics Committee opinion (2026)
This document discusses the ethical implications as well as the current limits and potential benefits of the use of preimplantation genetic testing for polygenic disorders.Practice Documents
ASRM Practice Documents have been developed to assist physicians with clinical decisions regarding the care of their patients.
Diagnosis and treatment of luteal phase deficiency: a committee opinion (2026)
Luteal phase deficiency (LPD) is a clinical diagnosis associated with abnormal luteal phase length of ≤10 days.
The International Glossary on Infertility and Fertility Care, 2025
Previous editions of the International Glossary on Infertility and Fertility Care established internationally recognized definitions related to clinical practice, research, and policy.
Intracytoplasmic sperm injection for nonmale factor indications: a Committee opinion (2026)
ICSI use extends beyond male infertility, raising questions about benefits when semen parameters meet WHO reference values.
Witnessing and protocol deviations in the in vitro fertilization and andrology laboratory: a committee opinion (2026)
A number of key misidentification risk points occur during an in vitro fertilization cycle in the laboratory that require robust witnessing.More Resources
ASRM Practice Documents

ASRM MAC Tool 2021
The ASRM Müllerian Anomaly Classification 2021 (MAC2021) includes cervical and vaginal anomalies and standardize terminology within an interactive tool format.

Coding Corner Q & A
The Coding Corner Q & A is a list of previously submitted and answered questions from ASRM members about coding. Answers are available to ASRM Members only.

EMR Shared Phrases/Template Library
This resource includes phrases shared by ASRM physician members to provide a template for individuals to create their own EMR phrases.
ASRM Ethics Opinions
Ethics Committee Reports are drafted by the members of the ASRM Ethics Committee on the tough ethical dilemmas of reproductive medicine.

COVID-19 Resources
A compendium of ASRM resources concerning the Novel Corona virus (SARS-COV-2) and COVID-19.

Patient Resources
ReproductiveFacts.org provides a wide range of information related to reproductive health and infertility through patient education fact sheets, infographics, videos, and other resources.