
Role of tubal surgery in the era of assisted reproductive technology: a committee opinion (2021)
Tubal disease accounts for 25%– 35% of female factor infertility, with more than half of the cases due o salpingitis (1). In addition, large studies report that up to 20%–30% of women regret having a tubal ligation (2–4). Thus, there is a need to determine the optimal treatment methods for patients with tubal-factor infertility. There are several surgical options for achieving patency in obstructed fallopian tubes or performing reparative tubal surgery. This document reviews these procedures and the factors that must be considered when deciding between surgical repair and in vitro fertilization (IVF).
DIAGNOSIS
A history of ectopic pregnancy, pelvic inflammatory disease, endometriosis, or prior pelvic surgery raises the index of suspicion for tubal-factor infertility. For patients with no risk factors, a negative chlamydia antibody test indicates that there is a <15% likelihood of tubal pathology (5). However, chlamydia antibody testing is limited by false positives from cross-reactivity with Chlamydia pneumoniae immuno- globulin G and does not distinguish be- tween remote and persistent infection, and it does not indicate whether the infection resulted in tubal damage (5). Therefore, hysterosalpingography (HSG) is the standard first-line test to evaluate tubal patency, especially if reparative surgery is planned (6).If HSG suggests patent tubes, tubal blockage is highly unlikely (7). However, in 60% of patients in whom HSG showed proximal tubal blockage, repeat HSG 1 month later showed tubal patency (8). A similar percentage of patients shown by HSG to have proximal tubal occlusion were found to have patent tubes on subsequent laparoscopy (7). In addition, 11 of 18 proximal tubes excised for blockage were found to be patent (9). Laparoscopy, considered as the gold standard for determining tubal patency, is not perfect; 1 study showed that 3% of patients with bilateral tubal occlusion subsequently conceived spontaneously (10). Hysterosalpingography may have a therapeutic effect, with higher fecundity rates reported for several months after the procedure (11) when tubal flushing was performed with oil-based contrast media (11, 12). The sensitivity of hysterosalpingo- contrast sonography for the determination of tubal patency ranges from 76% to 96%, although the specificity ranges from 67% to 100% (6). Upon the evaluation of the tubal patency with a saline-air device (hysterosalpingo-contrast sonography), concordance was found with hysterosalpingography in 85% of cases. Agreement with hysterosalpingography was excellent if the tubes were patent. The lack of agreement was with abnormal results. The sensitivity was 89.4% and specificity was 45.5% (13). The sensitivity of transvaginal hydrolaparoscopy in detecting tubal abnormalities was 100% and specificity was 22.2% (14). The hysteroscopy flow technique was associated with a sensitivity of 73.7% and specificity of 70.7%. The addition of air bubbles may improve both (15).
INTERPRETING OUTCOMES
The outcome of interest to infertile patients faced with the option of tubal surgery or IVF is the birth of healthy child or children, born 1 at a time. Outcomes after tubal surgery are generally reported in the medical literature on a per-patient basis highlighting the cumulative experience over the interval of follow-up, e.g., 6 months, 12 months, 2 years, 3 years, or more. In contrast, IVF is often reported on a per-cycle basis with cumulative outcomes after several treatment cycles that may or may not all occur over an identical length of time. Further complicating the interpretation is the element of aging. A patient using a frozen embryo years after an IVF cycle may have a higher single-month chance of success compared with another patient of the same age who chose to undergo tubal surgery. However, the surgical patient has had the benefit of multiple months of attempting pregnancy over those years. This document has been updated to help physicians interpret the existing data and counsel patients toward a treatment tailored to meet their individual circumstances, goals, and needs.GENERAL CONSIDERATIONS
Many variables need to be taken into consideration when counseling patients with tubal infertility regarding corrective surgery vs. IVF. The age of the patient, ovarian reserve, prior fertility, number of children desired, site and extent of the tubal disease, presence of other infertility factors, experience of the surgeon, and success rates of the IVF program are the most important. Patient preference, religious beliefs, cost, and insurance reimbursement also figure into the equation. In addition, a semen analysis should be performed early in the infertility investigation as the results may influence the management decision between tubal surgery and IVF.National assisted reproductive technology registry data from 2017 noted a 31.2% live-birth rate per cycle initiated in patients across all ages with tubal infertility, similar to the 34.1% rate overall (16). Meaningful success rates with the various tubal surgical procedures are largely lacking. Most of the published literature is from the surgeons with the greatest expertise. Their results may not be generalizable to less skilled or experienced surgeons. Furthermore, the results of tubal surgery and IVF are not directly comparable because surgical success is reported as pregnancy rate per patient, whereas IVF success rates are per cycle. As a result, there are no adequate trials comparing the pregnancy rates after tubal surgery vs. after IVF (17).
The advantages and disadvantages of IVF and tubal surgery need to be reviewed with the patient to assist her in decision making. The main advantages of IVF are good per-cycle success rates and the fact that it is less surgically invasive. Its disadvantages include cost (especially if >1 cycle is required), the need for frequent injections and monitoring for several weeks, and the risks of multiple pregnancy and ovarian hyperstimulation syndrome. It should be noted that current practice protocols can alleviate the risk of multiple pregnancy via single-embryo transfer, and there are evidence-based strategies to minimize the risk of ovarian hyperstimulation syndrome (18). IVF has been associated with a slightly higher incidence than unassisted conceptions of adverse perinatal outcomes in singleton infants, such as perinatal mortality, preterm delivery, low and very low birthweights, intrauterine growth restriction, and congenital malformations (19–24).
The advantages of tubal surgery are that it is a one-time, usually minimally invasive outpatient procedure. Patients may attempt conception every month without further intervention and may conceive more than once. The disadvantages are generalizable to surgeons with less skill and experience and include the risks for surgical complications, such as bleeding, infection, organ damage, and reaction to anesthesia. There is also postoperative discomfort during the short recovery phase. The risk of ectopic pregnancy is increased in patients having IVF for tubal disease, and it is higher after tubal surgery. In addition, for some patients, the success after tubal surgery may be significantly lower than that for IVF. Although the national registry reports clinic-specific statis- tics, outcomes for individual surgeons or centers are not re- ported. Therefore, only data from high-volume surgeons are reported in the literature, which may not apply to all centers. All these factors need to be considered when choosing the appropriate treatment strategy. To optimize pregnancy rates and reduce the risks, only those surgeons facile and experienced in laparoscopic and/or microsurgical techniques should attempt to perform corrective tubal surgery. The ideal patient candidate for tubal surgery is young, has no other significant infertility factors, and has tubal anatomy that is amenable to repair.
PROCEDURES FOR PROXIMAL TUBAL BLOCKAGE
Proximal tubal blockage accounts for 10%–25% of tubal dis- ease (1). It may be because of obstruction resulting from plugs of mucus and amorphous debris, spasm of the uterotubal ostium, or occlusion, which is a true anatomic blockage from fibrosis due to salpingitis isthmica nodosa, pelvic in- flammatory disease, or endometriosis. Unless the proximal blockage on HSG is clearly because of salpingitis isthmica nodosa, selective salpingography or tubal cannulation can be attempted.Tubal cannulation is accomplished using a coaxial catheter system under fluoroscopic guidance or using hysteroscopy with laparoscopic confirmation. An outer catheter is directed to the uterotubal ostium, and a selective salpingogram is performed. If tubal blockage is confirmed, a small inner catheter with a flexible guide wire is advanced through the proximal tube. Before performing this procedure, there should be confirmation of normal distal tubal anatomy at laparoscopy or by ultrasonography if the cannulation is performed by radiologic access.
If the obstruction is not overcome by tubal cannulation with gentle pressure, a true anatomic occlusion is assumed, and the procedure is terminated. Excision of the proximal tubes in cases of failed tubal cannulation revealed salpingitis isthmica nodosa, chronic salpingitis, or obliterative fibrosis in 93% of patients (25). In these cases, IVF is preferred over resection and microsurgical anastomosis. In vitro fertilization would also be the preferred treatment for proximal tubal blockage in older women and in the presence of significant male factor infertility. However, microsurgery may beconsidered after failed tubal cannulation if IVF is not an option for the patient, but it should be attempted only by those with appropriate training. A meta-analysis on tubal cannulation demonstrated that the pooled (both unilateral and bilateral obstruction) cumulative clinical pregnancy rates were 22.3% (95% confidence interval [CI]: 17.8%–27.8%) at 6 months and increased slowly to achieve 26.4% (95% CI: 23.0%–30.2%) at 12 months, 27.9% (95% CI: 24.9%–31.3%) at 36 months, and 28.5% (95% CI: 25.5%–31.8%) at 48 months. The pooled (unilateral and bilateral obstruction) live-birth rate was 22% (95% CI: 18%–26%) and the pooled ectopic pregnancy rate was 4% (95% CI: 3%–5%) (26). In women with bilateral obstruction, the clinical pregnancy rate was 27% (95% CI: 23%–32%) (26). Given that relatively few women conceive naturally >6–12 months post cannulation, subsequent alternative intervention can be initiated after 6 months to a year after successful cannulation.
Among those tubes for which patency is achieved, approximately one-third will reocclude (1, 27). The incidence of tubal perforation during tubal cannulation has been reported to be 3%–11%, without any clinical consequences (1). The optimal treatment of unilateral proximal tubal occlusion has not been determined. One study reported similar pregnancy rates with ovarian stimulation and intrauterine insemination in patients with untreated unilateral proximal tubal occlusion and in those with unexplained infertility (28). Therefore, there is no requirement for intervention with a unilateral proximal tubal obstruction with no distal abnormalities.
Tubal patency rates are similar with both fluoroscopic and hysteroscopic techniques (1). A recent meta-analysis con- firms this finding, with pooled pregnancy rates of 31% for the hysteroscopic approach vs. 26% for the fluoroscopic (26). The difference in pregnancy rates between these 2 methods was not statistically significant (P¼ .596). Because the hysteroscopy is combined with laparoscopy, this could be the opportunity to diagnose and treat other pelvic pathology. Because tubal cannulation is a minor procedure with results comparable to those of microsurgical resection and anastomosis, it should be the treatment of choice.
SURGERY FOR DISTAL TUBAL DISEASE— GOOD PROGNOSIS
The decision to repair or remove fallopian tubes with distal disease is usually made intraoperatively on the basis of the prognosis for an intrauterine pregnancy. Distal tubal disease includes hydrosalpinges, fimbrial phimosis, and peritubal adhesions. Hydrosalpinges are completely occluded, whereas fimbrial agglutination by adhesions results in a narrow phimotic tubal opening. Both conditions are usually because of pelvic inflammatory disease but may also result from peritonitis or previous surgery. Patients with a good prognosis have limited filmy adnexal adhesions, mildly dilated tubes (<3 cm) with thin and pliable walls, and a lush endosalpinx with the preservation of the mucosal folds (29). Peritubal adhesions impair the ability of intrinsically normal tubes to capture an oocyte by mechanically interfering with the anatomic relationship between the distal fallopian tube and the ovary. One study of 147 patients with peritubal adhesions diagnosed at laparotomy reported a cumulative pregnancy rate of 40% at 12 months after adhesiolysis vs. 8% in an untreated group (30).Laparoscopic neosalpingostomy and fimbrioplasty are performed by opening a hydrosalpinx or increasing the opening for fimbrial phimosis, respectively. The fimbria are then everted and secured to the tubal serosa with sutures or electrosurgery (31). Pregnancy rates after these procedures depend on the degree of tubal disease and are more favorable with good-prognosis patients (32, 33). Intrauterine and ectopic pregnancy rates after neosalpingostomy for mild hydrosalpinges range from 58% to 77% and from 2% to 8%, respectively (32). For severe disease, these values were 0%–22% and 0%–17%, respectively (32). In a more recent retrospective study from a single center evaluating 434 patients, the clinical pregnancy rates were significantly different on the basis of the stage of tubal disease: 43% in stage 1, 33.6% in stage 2, 19.5% in stage 3, and 13.8% in stage 4, with half of the patients conceiving within 11 months and 75% within 21 months. The ectopic pregnancy rate ranged from 5.6% to 11.4% (34, 35). Irreversible deciliation of the endosalpinx after an episode of salpingitis is likely responsible for the discrepancy between the patency rates and pregnancy rates after neosalpingostomy.
The fimbrioplasty procedure to open the tube more widely is virtually identical to neosalpingostomy. Neosalpingostomy and fimbrioplasty should be done only by laparoscopy, because the results are comparable to those of laparotomy, but with less risk (6, 36). Although IVF is preferred over salpingostomy for mild hydrosalpinges in older women and for those with male factor infertility or other infertility fac- tors, salpingostomy before IVF may improve the subsequent likelihood of success of IVF while still giving the patient the option to attempt spontaneous conception. Reparative surgery is not appropriate for women with severe disease or those with both proximal and distal occlusion. Patients with poor-prognosis hydrosalpinges are better served by salpingectomy followed by IVF. Patients should be consented preoperatively for both salpingostomy as well as salpingectomy so that the most appropriate procedure can be performed on the basis of the extent of tubal disease. The patient should be counseled that postoperative reocclusion may occur, necessitating an additional surgical procedure to perform a salpingectomy.
SURGERY FOR DISTAL TUBAL BLOCKAGE— POOR PROGNOSIS
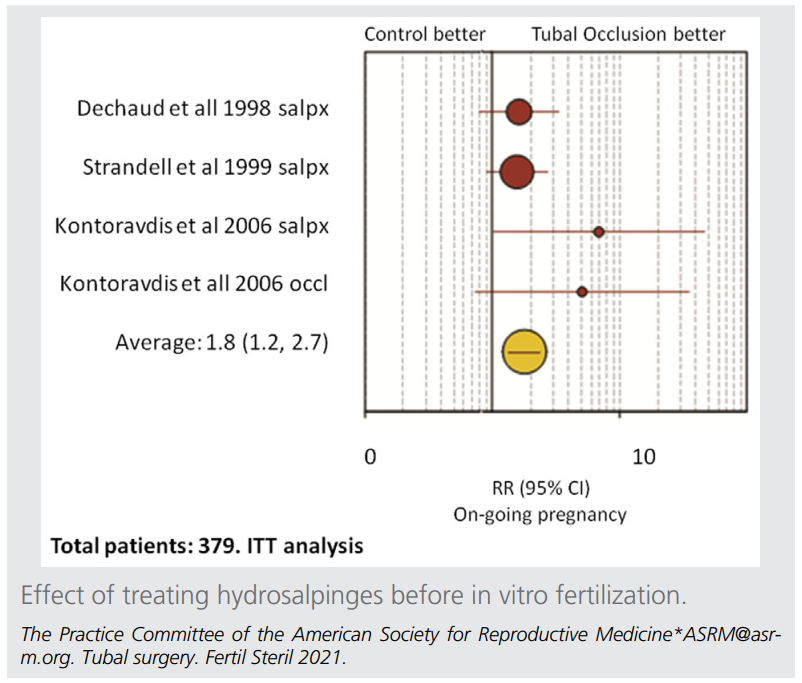
Patients having a poor prognosis have extensive dense peritubal adhesions, largely dilated tubes with thick fibrotic walls, and/or sparse or absent luminal mucosa. Laparoscopic salpingectomy is indicated in patients with hydrosalpinges of poor prognosis as they have a detrimental effect on IVF success rates. Two meta-analyses have shown that the pregnancy, im- plantation, and delivery rates were approximately 50% lower in the presence of hydrosalpinges (37, 38). This finding may be because of mechanical flushing of the embryos from the uterine cavity, decreased endometrial receptivity, or a direct embryotoxic effect (39). Patients with hydrosalpinges visible on ultrasound may be more significantly affected (40, 41). Randomized clinical trials comparing pregnancy rates and outcomes with IVF for women with hydrosalpinges, with or without prior laparoscopic salpingectomy, reported that salpingectomy restores the rates of pregnancy and live birth to levels similar to those of women without hydrosalpinx (40, 42, 43) (Fig. 1). A meta-analysis concluded that laparoscopic salpingectomy or tubal occlusion should be considered before IVF for women with communicating hydrosalpinges (44). Even patients with unilateral hydrosalpinx have been shown to have lower pregnancy rates with IVF (45, 46). Unilateral salpingectomy resulted in a significant improvement in IVF pregnancy rates in these patients (40, 47). It should also be noted that there have been several case reports of spontaneous pregnancy after salpingectomy for a unilateral hydrosalpinx (40, 48–50). In the largest series of 25 patients, the mean duration of infertility was 3 years and 22 (88%) patients conceived spontaneously, within a mean of 5.6 months postoperatively with no ectopic pregnancies (50).Although salpingectomy and even tubal ligation have been implicated as causes of subsequent diminished ovarian reserve (51), a study of IVF before and after salpingectomy for ectopic pregnancy found no significant differences in dose or duration of gonadotropins used or peak estradiol levels (52). Furthermore, there was no difference in the number of oocytes retrieved or embryo quality between cycles or between the ovaries (52). The preponderance of evidence suggests that salpingectomy for hydrosalpinges also did not result in differences in ovarian stimulation or IVF parameters before or after surgery (53). These data only report clinical pregnancy rates and not live-birth rates.
Proximal tubal obstruction may be an alternative to salpingectomy. In 2 randomized clinical trials, researchers re- ported that proximal tubal occlusion was also effective in restoring IVF pregnancy rates in women with hydrosalpinx (42, 54). There is a theoretical concern that proximal occlusion may lead to an increase in the size of the hydrosalpinx, as the fluid can no longer drain through the uterus. For this reason, consideration may be given to widely fenestrating the hydrosalpinges at the time of proximal occlusion.
Although the present literature clearly points to an advantage of removing the hydrosalpinx before IVF, this population is at an inherently higher surgical risk because of the history of pelvic infection and/or adhesive disease. Because of the desire to avoid the added physical, financial, and emotion burden of surgery, new research has focused on minimally invasive methods of relieving the deleterious effects of hydrosalpinx, such as aspiration and sclerotherapy.
Ultrasound-guided aspiration of hydrosalpinges at the time of oocyte retrieval yielded conflicting results in 2 small retrospective studies (55, 56). A randomized study comparing ultrasound-guided aspiration with a nontreated control reported significantly higher biochemical pregnancy rates with aspiration with a trend for increased clinical pregnancy rates after aspiration vs. control (at 31.3% [10/32] vs. 17.6% [6/34], respectively [relative risk ¼ 1.8 {0.8, 4.3}, P¼ .20]) (57).
However, a retrospective study evaluating a total of 598 IVF embryo transfer cycles for tubal disease with 4 groups consisting of patients with previously diagnosed hydrosalpinx with aspiration at the time of retrieval; hydrosalpinx occurring during stimulation also aspirated at the time of retrieval; hydrosalpinx with no intervention; and the control group of patients without hydrosalpinx revealed a benefit of aspiration to those who were diagnosed with hydrosalpinx during stimulation but not for aspiration of hydrosalpinx that was present prior (58).
Simple aspiration, either at the time of diagnosis or the time of retrieval, had been questioned as ineffective secondary to the high rate of fluid recurrence. Consequently, sclerotherapy, using instillation of ethanol to contract, sclerose, and decrease secretory function of the tube, has been postulated to help prevent the recurrence of toxic hydrosalpinx fluid (59). A meta-analysis of 10 studies found a similar recurrence rate of fluid collection between hydrosalpinx aspiration and sclerotherapy (approximately 20%–30%). However, when compared with salpingectomy, hydrosalpinx sclerotherapy showed no difference in clinical pregnancy or miscarriage rates whereas aspiration alone had lower clinical pregnancy and higher miscarriage rates. Alternatively, compared with no intervention, simple aspiration resulted in higher clinical pregnancy rates but a similar miscarriage rate (60). Therefore, it appears that intervention to decompress the hydrosalpinx by ultrasound- guided aspiration is superior to no intervention at all, but sclerotherapy may be a superior option and salpingectomy remains the gold standard to optimize reproductive options in the management of hydrosalpinx before IVF.
Regarding the surgical approach, open tubal surgery has all but been abandoned for minimally invasive methods, except for the most complicated of surgical histories because of the shorter recovery time, less blood loss, fewer complications, and similar completion rates (6, 36). The addition of a surgical robot or tubal surgery can alleviate the need for a skilled surgical assistant and add dexterity for suturing; how- ever, it adds little utility in the hands of a skilled laparoscopic surgeon for uncomplicated distal tubal surgery and may add extra cost.
Figure 1
SURGERY FOR STERILIZATION REVERSAL
For women with a prior tubal ligation who wish to conceive, the discussion regarding tubal anastomosis vs. IVF should be individualized. Patient age, partner semen quality, surgical technique that was used to perform the sterilization, expense, chance of success, and reproductive preferences are essential elements in decision-making. This population is usually otherwise fertile and has better success rates after surgery than patients with tubal pathology. When compared with national IVF success rates by age, women with prior tubal ligation may also have a better prognosis with IVF. The reversal of tubal ligation is achieved by opening the occluded ends of the proximal and distal segments and anastomosing them with fine monofilament sutures using magnification and microsurgical techniques. Anastomoses are typically achieved with a 2-layer technique, including 4 interrupted sutures placed in the muscularis followed by the reapproximation of the overlying serosa.Laparotomic surgery has been largely replaced with minimally invasive techniques, including outpatient minilaparotomy microsurgical anastomosis as well as laparoscopic and robotic approaches (61). Prospective comparisons with laparotomy and randomized studies comparing minimally invasive methods are lacking. Case series and retrospective cohort studies demonstrate equivalent pregnancy rates among microsurgical, laparoscopic, and robotic tubal anastomoses. Pooled pregnancy rates for these techniques in a 2017 systematic review ranged from 65%–68% (62), with success being most significantly associated with patient age. The method of prior tubal ligation also appears to predict successful anastomosis. The reversal of sterilization procedures per- formed with rings or clips results in higher pregnancy rates than for sterilization performed via ligation/resection or coagulation (63).
Despite comparable pregnancy and ectopic rates, case times for minimally invasive tubal reversal are longer than that with an open approach (62). The main challenge in laparoscopic anastomosis procedures is the technical demands of laparoscopic suturing. Only surgeons who are very facile with laparoscopic suturing and who have experience and training in tubal microsurgery should attempt this procedure. Transvaginal natural orifice surgery (64) offers an alternative means of accessing the tubes for reversal procedures; however, the requisite skill set in correct approximation of the tubes remains the same.
Robotic assistance lessens the technical challenges of a laparoscopic approach but with notable tradeoffs in cost and operative time (62). Although the pregnancy rates with robot are similar to those achieved with open tubal anastomosis, 2 small trials demonstrated shorter recovery times and significantly higher cost and operative time for robotic cases (61, 65). In addition to the use of robotics, several other techniques have been proposed to circumvent the challenges of laparoscopic suturing. Both single-stitch and single-tube approaches (66) have been described in addition to the use of microstaplers, fine barbed suture, titanium clips, and fibrin glue. The goal of laparoscopic surgery should be to duplicate established open procedures and shortcuts may compromise typical clinical results. There are no comparative trials evaluating the use of these techniques vs. standard approaches.
Patient age is consistently the most significant prognostic factor in the chance for successful sterilization reversal. In a series of >6,500 women undergoing tubal anastomosis, women <30 years at the time of the reversal had a pregnancy rate of 88%, with pregnancy and live-birth rates significantly decreasing with increasing age (63). Success after tubal reversal is not restricted to younger women; pooling pregnancy rates for all subjects <40 years, a retrospective single-center study reported cumulative intrauterine pregnancy rates of >90% within 2 years of microsurgical reversal of tubal sterilization (67). In women aged 40–45 years, a multicenter study with 78 women reported a 45% pregnancy rate; the reported miscarriage rate of 26% was likely related to the advanced age of the women in the study (68). Other prognostic factors which are thought to predict success include final tubal length and the site of tubal reapproximation (e.g., isthmic-isthmic reversals may have greater success than ampullary or cornual segments). Surgeons may wish to defer reversal procedures in instances of final tubal lengths predicted to be <4 cm, significant tubo-ovarian adhesions, advanced endometriosis, or recognized significant male factor infertility. If no pregnancy occurs within 6 months, an assessment of tubal patency is suggested.
When considering sterilization reversal vs. IVF, increased ectopic rates after tubal reversal surgery are a relevant consideration. The rate of ectopic pregnancy after tubal anastomosis was reported as 4%–8% vs. 1.4% for IVF (62, 69). Women who elect tubal anastomosis require early surveillance with the occurrence of a positive pregnancy test.
For women <37 years of age, cumulative delivery rates were higher for women undergoing tubal anastomosis than those for women undergoing IVF (72% vs. 52%, respectively), with costs in the tubal reversal group that were nearly half as much as those in the IVF group (70). There was no significant difference in delivery rates in women aged >37 years. Cost comparisons and decision-tree modeling has determined that the average cost per pregnancy is only higher for tubal anastomosis compared with IVF in women >40 years old (71). An ongoing concern in the provision of high-quality tubal anastomosis is the current lack of adequate instruction in laparoscopic and microsurgical techniques (72). Trainees in minimally invasive gynecology and reproductive endocrinology may not have received the necessary experience or technical skills to successfully perform this procedure; in this context, predicted ectopic and live-birth rates may vary. In one study, 43% of reproductive endocrinology fellows reported that they had not performed a tubal anastomosis as the primary surgeon (73). Opportunities should be expanded to train the next generation of reproductive surgeons in mastering this cost-effective approach for women who wish to achieve spontaneous fertility after tubal sterilization.
SUMMARY
- Factors to be considered when counseling patients with tubal infertility regarding corrective surgery or IVF include the age of the woman and ovarian reserve, number and quality of sperm in the ejaculate, number of children desired, site and extent of tubal disease, presence of other infertility factors, risk of ectopic pregnancy and other com- plications, experience of the surgeon, success rates of the IVF program, cost, and patient preference.
- Most IVF pregnancies, even in cumulative studies, happen within 1 year. In contrast, many surgical studies have high cumulative numbers but the time to delivery is substantially longer.
- There are no adequate trials comparing pregnancy rates of tubal surgery with IVF. However, IVF has a higher per-cycle pregnancy rate. Tubal anastomosis for the reversal of tubal sterilization has a significantly higher cumulative pregnancy rate than that of IVF.
- Laparoscopic salpingectomy or proximal tubal ligation overcomes the detrimental effect of hydrosalpinges on IVF pregnancy rates in patients who are not candidates for corrective tubal surgery.
- Aspiration of a hydrosalpinx with or without sclerotherapy may be superior to no treatment at all, but further studies are needed.
CONCLUSIONS
- HSG should be considered the standard first-line test to assess tubal patency, but it is limited by false-positive diagnoses of proximal tubal blockage.
- Tubal cannulation for proximal tubal obstruction in young women with no other significant infertility factors is recommended.
- Laparoscopic fimbrioplasty or neosalpingostomy is recommended for the treatment of mild hydrosalpinges in young women with no other significant infertility factors.
- Laparoscopic salpingectomy should be used for proximal tubal occlusion in cases of surgically irreparable hydrosalpinges to improve IVF pregnancy rates.
- Microsurgical anastomosis is the recommended technique for tubal ligation reversal.
Acknowledgments: This report was developed under the direction of the Practice Committee of the American Society for Reproductive Medicine (formerly The American Fertility Society) as a service to its members and other practicing clinicians. Although this document reflects appropriate management of a problem encountered in the practice of reproductive medicine, it is not intended to be the only approved standard of practice or to dictate an exclusive course of treatment. Other plans of management may be appropriate, taking into account the needs of the individual patient, available resources, and institutional or clinical practice limitations. The Practice Committee and the Board of Directors of the American Society for Reproductive Medicine (ASRM) have approved this report.
This document was reviewed by ASRM members and their input was considered in the preparation of the final document. The following members of the ASRM Practice Committee participated in the development of this document: Alan Penzias, M.D.; Ricardo Azziz, M.D., M.P.H., M.B.A.; Kristin Bendikson, M.D.; Tommaso Falcone, M.D.; Karl Hansen, M.D., Ph.D.; Micah Hill, D.O.; Sangita Jindal, Ph.D.; Suleena Kalra, M.D., M.S.C.E.; Jennifer Mersereau, M.D.; Richard Reindollar, M.D.; Chevis N. Shannon, Dr.P.H., M.P.H., M.B.A.; Anne Steiner, M.D., M.P.H.: Dale Stovall, M.D.; Cigdem Tanrikut, M.D.; Hugh Tay- lor, M.D.; and Belinda Yauger, M.D.. The Practice Committee acknowledges the special contribution of John Petrozza, M.D.; Rebecca Flyckt, M.D.; Linnea Goodman, M.D.; and Rony Elias, M.D. in the preparation of this document. All Committee members disclosed commercial and financial relationships with manufacturers or distributors of goods or ser- vices used to treat patients. Members of the Committee who were found to have conflicts of interest on the basis of the relationships disclosed did not participate in the discussion or development of this document.
REFERENCES
- Honore GM, Holden AE, Schenken RS. Pathophysiology and management of proximal tubal blockage. Fertil Steril 1999;71:785–95.
- Borrero SB, Reeves MF, Schwarz EB, Bost JE, Creinin MD, Ibrahim SA. Race, insurance status, and desire for tubal sterilization reversal. Fertil Steril 2008; 90:272–7.
- Schmidt JE, Hillis SD, Marchbanks PA, Jeng G, Peterson HB. Requesting in- formation about and obtaining reversal after tubal sterilization: findings from the U.S. Collaborative Review of Sterilization. Fertil Steril 2000;74: 892–8.
- Chi IC, Jones DB. Incidence, risk factors, and prevention of poststerilization regret in women: an updated international review from an epidemiological perspective. Obstet Gynecol Surv 1994;49:722–32.
- den Hartog JE, Morr'e SA, Land JA. Chlamydia trachomatis-associated tubal factor subfertility: immunogenetic aspects and serological screening. Hum Reprod Update 2006;12:719–30.
- Infertility workup for the women’s health specialist: ACOG committee opinion, number 781. Obstet Gynecol 2019;133:e377–84.
- Evers JL, Land JA, Mol BW. Evidence-based medicine for diagnostic questions. Semin Reprod Med 2003;21:9–15.
- Dessole S, Meloni GB, Capobianco G, Manzoni MA, Ambrosini G, Canalis GC. A second hysterosalpingography reduces the use of selective technique for treatment of a proximal tubal obstruction. Fertil Steril 2000; 73:1037–9.
- Sulak PJ, Letterie GS, Coddington CC, Hayslip CC, Woodward JE, Klein TA. Histology of proximal tubal occlusion. Fertil Steril 1987;48:437–40.
- Mol BW, Collins JA, Burrows EA, van der Veen F, Bossuyt PM. Comparison of hysterosalpingography and laparoscopy in predicting fertility outcome. Hum Reprod 1999;14:1237–42.
- Mohiyiddeen L, Hardiman A, Fitzgerald C, Hughes E, Mol BW, Johnson N, et al. Tubal flushing for subfertility. Cochrane Database Syst Rev 2015; 2015:CD003718.
- Dreyer K, van Rijswijk J, Mijatovic V, Goddijn M, Verhoeve HR, van Rooij IAJ, et al. Oil-based or water-based contrast for hysterosalpingography in infer- tile women. N Engl J Med 2017;376:2043–52.
- Robertshaw IM, Sroga JM, Batcheller AE, Martinez AM, Winter TC, Sinning K, et al. Hysterosalpingo-contrast sonography with a saline-air de- vice is equivalent to hysterosalpingography only in the presence of tubal patency. J Ultrasound Med 2016;35:1215–22.
- Tros R, van Kessel M, Oosterhuis J, Kuchenbecker W, Bongers M, Mol B, et al. Transvaginal hydrolaparoscopy and laparoscopy. Reprod Biomed On- line 2020;40:105–12.
- Hager M, Ott J, Holzer I, Seemann R, Kurz C, Parry JP. Hysteroscopic assessment of tubal patency: a randomized comparison between the Flow and Parryscope techniques. J Minim Invasive Gynecol 2020;27:1552–7.e1.
- Society for Assisted Reproductive Technology. Clinic summary report. Avail- able at: https://www.sartcorsonline.com/rptCSR_PublicMultYear.aspx?Clin- icPKID¼0. Accessed November 3, 2020.
- Chua SJ, Akande VA, Mol BW. Surgery for tubal infertility. Cochrane Data- base Syst Rev 2017;1:CD006415.
- Practice Committee of the American Society for Reproductive Medicine. Prevention and treatment of moderate and severe ovarian hyperstimulation syndrome: a guideline. Fertil Steril 2016;106:1634–47.
- Hansen M, Bower C, Milne E, de Klerk N, Kurinczuk JJ. Assisted reproductive technologies and the risk of birth defects—a systematic review. Hum Reprod 2005;20:328–38.
- McDonald SD, Murphy K, Beyene J, Ohlsson A. Perinatel outcomes of singleton pregnancies achieved by in vitro fertilization: a systematic review and meta-analysis. J Obstet Gynaecol Can 2005;27:449–59.
- Jackson RA, Gibson KA, Wu YW, Croughan MS. Perinatal outcomes in singletons following in vitro fertilization: a meta-analysis. Obstet Gynecol 2004; 103:551–63.
- Kallen B, Finnstro€m O, Lindam A, Nilsson E, Nygren KG, Otterblad PO. Congenital malformations in infants born after in vitro fertilization in Sweden. Birth Defects Res A Clin Mol Teratol 2010;88:137–43.
- El-Chaar D, Yang Q, Gao J, Bottomley J, Leader A, Wen SW, et al. Risk of birth defects increased in pregnancies conceived by assisted human repro- duction. Fertil Steril 2009;92:1557–61.
- Rizzuto I, Behrens RF, Smith LA. Risk of ovarian cancer in women treated with ovarian stimulating drugs for infertility. Cochrane Database Syst Rev 2019;6:CD008215.
- Letterie GS, Sakas EL. Histology of proximal tubal obstruction in cases of un- successful tubal canalization. Fertil Steril 1991;56:831–5.
- De Silva PM, Chu JJ, Gallos ID, Vidyasagar AT, Robinson L, Coomarasamy A. tion: a systematic review and meta-analysis. Hum Reprod 2017;32:836–52.
- Pinto AB, Hovsepian DM, Wattanakumtornkul S, Pilgram TK. Pregnancy out- comes after fallopian tube recanalization: oil-based versus water-soluble contrast agents. J Vasc Interv Radiol 2003;14:69–74.
- Farhi J, Ben-Haroush A, Lande Y, Fisch B. Role of treatment with ovarian stimulation and intrauterine insemination in women with unilateral tubal oc- clusion diagnosed by hysterosalpingography. Fertil Steril 2007;88:396–400.
- American Fertility Society. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Mullerian anomalies and intrauterine adhesions. Fertil Steril 1988;49:944–55.
- Tulandi T, Collins JA, Burrows E, Jarrell JF, McInnes RA, Wrixon W, et al. Treatment-dependent and treatment-independent pregnancy among women with periadnexal adhesions. Am J Obstet Gynecol 1990;162: 354–7.
- Goldberg JM, Falcone T, Diamond MP. Current controversies in tubal dis- ease, endometriosis, and pelvic adhesion. Fertil Steril 2019;112:417–25.
- Nackley AC, Muasher SJ. The significance of hydrosalpinx in in vitro fertiliza- tion. Fertil Steril 1998;69:373–84.
- Milingos SD, Kallipolitis GK, Loutradis DC, Liapi AG, Hassan EA, Mavrommatis CG, et al. Laparoscopic treatment of hydrosalpinx: factors affecting pregnancy rates. J Am Assoc Gynecol Laparosc 2000;7:355–61.
- Audebert A, Pouly JL, Bonifacie B, Chadi Yazbeck C. Laparoscopic surgery for distal tubal occlusions: lessons learned from a historical series of 434 cases. Fertil Steril 2014;102:1203–8.
- Mage G, Pouly JL, de Jolini'ere JB, Chabrand S, Riouallon A, Bruhat MA. A preoperative classification to predict the intrauterine and ectopic pregnancy rates after distal tubal microsurgery. Fertil Steril 1986;46:807–10.
- Bontis JN, Theodoridis TD. Laparoscopic management of hydrosalpinx. Ann N Y Acad Sci 2006;1092:199–210.
- Zeyneloglu HB, Arici A, Olive D. Adverse effects of hydrosalpinx on pregnancy rates after in vitro fertilization-embryo transfer. Fertil Steril 1998;70: 492–9.
- Camus E, Poncelet C, Goffinet F, Wainer B, Merlet F, Nisand I, et al. Preg- nancy rates after in-vitro fertilization in cases of tubal infertility with and without hydrosalpinx: a meta-analysis of published comparative studies. Hum Reprod 1999;14:1243–9.
- Practice Committee of the American Society for Reproductive Medicine. Salpingectomy for hydrosalpinx prior to in vitro fertilization. Fertil Steril 2008; 90(Suppl 5):S66–8.
- Strandell A, Lindhard A, Waldenstro€m U, Thorburn J, Janson PO, Hamberger L. Hydrosalpinx and IVF outcome: a prospective, randomized multicentre trial in Scandinavia on salpingectomy prior to IVF. Hum Reprod 1999;14:2762–9.
- de Wit W, Gowrising CJ, Kuik DJ, Lens JW, Schats R. Only hydrosalpinges visible on ultrasound are associated with reduced implantation and preg- nancy rates after in-vitro fertilization. Hum Reprod 1998;13:1696–701.
- D'echaud H, Daur'es JP, Arnal F, Humeau C, H'edon B. Does previous salpingectomy improve implantation and pregnancy rates in patients with severe tubal factor infertility who are undergoing in vitro fertilization? A pilot pro- spective randomized study. Fertil Steril 1998;69:1020–5.
- Kontoravdis A, Makrakis E, Pantos K, Botsis D, Deligeoroglou E, Creatsas G. Proximal tubal occlusion and salpingectomy result in similar improvement in in vitro fertilization outcome in patients with hydrosalpinx. Fertil Steril 2006; 86:1642–9.
- Johnson N, van Voorst S, Sowter MC, Strandell A, Mol BW. Surgical treat- ment for tubal disease in women due to undergo in vitro fertilisation. Cochrane Database Syst Rev 2010;2010:CD002125.
- Kassabji M, Sims JA, Butler L, Muasher SJ. Reduced pregnancy outcome in patients with unilateral or bilateral hydrosalpinx after in vitro fertilization. Eur J Obstet Gynecol Reprod Biol 1994;56:129–32.
- Murray DL, Sagoskin AW, Widra EA, Levy MJ. The adverse effect of hydro- salpinges on in vitro fertilization pregnancy rates and the benefit of surgical correction. Fertil Steril 1998;69:41–5.
- Shelton KE, Butler L, Toner JP, Oehninger S, Muasher SJ. Salpingectomy im- proves the pregnancy rate in in-vitro fertilization patients with hydrosalpinx. Hum Reprod 1996;11:523–5.
- Choe J, Check JH. Salpingectomy for unilateral hydrosalpinx may improve in vivo fecundity. Gynecol Obstet Invest 1999;48:285–7.
- Aboulghar MA, Mansour RT, Serour GI. Spontaneous intrauterine preg- nancy following salpingectomy for a unilateral hydrosalpinx. Hum Reprod 2002;17:1099–100.
- Sagoskin AW, Lessey BA, Mottla GL, Richter KS, Chetkowski RJ, Chang AS, et al. Salpingectomy or proximal tubal occlusion of unilateral hydrosalpinx increases the potential for spontaneous pregnancy. Hum Reprod 2003;18: 2634–7.
- Chan CC, Ng EH, Li CF, Ho PC. Impaired ovarian blood flow and reduced antral follicle count following laparoscopic salpingectomy for ectopic pregnancy. Hum Reprod 2003;18:2175–80.
- Dar P, Sachs GS, Strassburger D, Bukovsky I, Arieli S. Ovarian function before and after salpingectomy in artificial reproductive technology patients. Hum Reprod 2000;15:142–4.
- Strandell A, Lindhard A, Waldenstro€m U, Thorburn J. Prophylactic salpingectomy does not impair the ovarian response in IVF treatment. Hum Reprod 2001;16:1135–9.
- Stadtmauer LA, Riehl RM, Toma SK, Talbert LM. Cauterization of hydrosal- pinges before in vitro fertilization is an effective surgical treatment associated with improved pregnancy rates. Am J Obstet Gynecol 2000;183: 367–71.
- Sowter MC, Akande VA, Williams JA, Hull MG. Is the outcome of in-vitro fertilization and embryo transfer treatment improved by spontaneous or surgical drainage of a hydrosalpinx? Hum Reprod 1997;12:2147–50.
- Van Voorhis BJ, Sparks AE, Syrop CH, Stovall DW. Ultrasound-guided aspiration of hydrosalpinges is associated with improved pregnancy and im- plantation rates after in-vitro fertilization cycles. Hum Reprod 1998;13: 736–9.
- Hammadieh N, Coomarasamy A, Ola B, Papaioannou S, Afnan M, Sharif K. Ultrasound-guided hydrosalpinx aspiration during oocyte collection im- proves pregnancy outcome in IVF: a randomized controlled trial. Hum Re- prod 2008;23:1113–7.
- Zhou Y, Jiang H, Zhang WX, Ni F, Wang XM, Song XM. Ultrasound-guided aspiration of hydrosalpinx occurring during controlled ovarian hyperstimulation could improve clinical outcome of in vitro fertilization-embryo transfer. J Obstet Gynaecol Res 2016;42:960–5.
- Song XM, Jiang H, Zhang WX, Zhou Y, Ni F, Wang XM. Ultrasound sclerotherapy pretreatment could obtain a similar effect to surgical intervention on improving the outcomes of in vitro fertilization for patients with hydrosal- pinx. J Obstet Gynaecol Res 2017;43:122–7.
- Cohen A, Almog B, Tulandi T. Hydrosalpinx sclerotherapy before in vitro fertilization: systematic review and meta-analysis. J Minim Invasive Gynecol 2018;25:600–7.
- Rodgers AK, Goldberg JM, Hammel JP, Falcone T. Tubal anastomosis by robotic compared with outpatient minilaparotomy. Obstet Gynecol 2007;109: 1375–80.
- van Seeters JAH, Chua SJ, Mol BWJ, Koks CAM. Tubal anastomosis after previous sterilization: a systematic review. Hum Reprod Update 2017;23:358–70.
- Berger GS, Thorp JM Jr, Weaver MA. Effectiveness of bilateral tubotubal anastomosis in a large outpatient population. Hum Reprod 2016;31: 1120–5.
- Liu J, Bardawil E, Lin Q, Liang B, Wang W, Wu C, et al. Transvaginal natural orifice transluminal endoscopic surgery tubal reanastomosis: a novel route for tubal surgery. Fertil Steril 2018;110:182.
- Dharia Patel SP, Steinkampf MP, Whitten SJ, Malizia BA. Robotic tubal anas- tomosis: surgical technique and cost effectiveness. Fertil Steril 2008;90: 1175–9.
- Paul PG, Bhosale SA, Khan S, Talwar P, Kandhari D, Kaur H. Fertility outcome in laparoscopic single tube reanastomosis. J Reprod Med 2015;60:30–6.
- Kim JD, Kim KS, Doo JK, Rhyeu CH. A report on 387 cases of microsurgical tubal reversals. Fertil Steril 1997;68:875–80.
- Trimbos-Kemper TC. Reversal of sterilization in women over 40 years of age: a multicenter survey in the Netherlands. Fertil Steril 1990;53:575–7.
- Santos-Ribeiro S, Tournaye H, Polyzos NP. Trends in ectopic pregnancy rates following assisted reproductive technologies in the UK: a 12-year nation- wide analysis including 160 000 pregnancies. Hum Reprod 2016;31:393– 402.
- Boeckxstaens A, Devroey P, Collins J, Tournaye H. Getting pregnant af- ter tubal sterilization: surgical reversal or IVF? Hum Reprod 2007;22: 2660–4.
- Messinger LB, Alford CE, Csokmay JM, Henne MB, Mumford SL, Segars JH, et al. Cost and efficacy comparison of in vitro fertilization and tubal anastomosis for women after tubal ligation. Fertil Steril 2015; 104:32–8.e4.
- Estes SJ, Bhagavath B, Lindheim SR. Tubal anastomosis: once in a blue moon? Fertil Steril 2018;110:64–5.
- Armstrong A, Neithardt AB, Alvero R, Sharara FI, Bush M, Segars J. The role of fallopian tube anastomosis in training fellows: a survey of current reproductive endocrinology fellows and practitioners. Fertil Steril 2004; 82:495–7.
Practice Documents
ASRM Practice Documents have been developed to assist physicians with clinical decisions regarding the care of their patients.
Tobacco or marijuana use and infertility: a committee opinion (2023)
In the United States, approximately 21% of adults report some form of tobacco use, although 18% report marijuana use.
Prevention of moderate and severe ovarian hyperstimulation syndrome: a guideline (2023)
Ovarian hyperstimulation syndrome is a serious complication associatedwith assisted reproductive technology.
Definition of infertility: a committee opinion (2023)
‘‘Infertility’’ is a disease, condition, or status characterized by several factors.
Clinical management of mosaic results from preimplantation genetic testing for aneuploidy of blastocysts: a committee opinion (2023)
This document incorporates studies about mosaic embryo transfer and provides evidence-based considerations for embryos with mosaic results on PGT-A.More Resources

ASRM MAC Tool 2021
The ASRM Müllerian Anomaly Classification 2021 (MAC2021) includes cervical and vaginal anomalies and standardize terminology within an interactive tool format.

EMR Shared Phrases/Template Library
This resource includes phrases shared by ASRM physician members to provide a template for individuals to create their own EMR phrases.
ASRM Practice Documents

ASRM Ethics Opinions
Ethics Committee Reports are drafted by the members of the ASRM Ethics Committee on the tough ethical dilemmas of reproductive medicine.

Coding Corner Q & A
The Coding Corner Q & A is a list of previously submitted and answered questions from ASRM members about coding. Answers are available to ASRM Members only.

COVID-19 Resources
A compendium of ASRM resources concerning the Novel Corona virus (SARS-COV-2) and COVID-19.

Patient Resources
ReproductiveFacts.org provides a wide range of information related to reproductive health and infertility through patient education fact sheets, infographics, videos, and other resources.
Topic Resources
Coding of identification of sperm in aspirate
During vasovasostomy/vasoepididyostomy procedures, our surgeons perform intra-op sperm identification from aspirate View the AnswerCoding for fluid aspiration during HSG
For physician-performed sonoHSG (58340& 76831) and uterine aspiration due to fluid, can an additional code for the aspiration be billed? View the AnswerBilling 58558 together with 58560
Can CPT codes 58558 and 58560 be billed together? Also, can 58560 be billed with place of service 11? View the AnswerASRM Today: ASRM Training Surgical Research Fund with Dr. Joseph Sanfilippo and Holly Hilton
In this episode from ASRM 2023 in New Orleans, I'm talking with Dr. Joseph Sanfilippo and Holly Hilton about the ASRM Training Surgical Research Fund. Listen to the EpisodeEndometrioma
Surgery was performed under anesthesia for Aspiration of right hyrosalpinx fluid and right endometrioma. View the AnswerASRM Announces Establishment Of Joseph Sanfilippo, MD, MBA In Training-Surgical Research Fund
ASRM announces the establishment of a new endowment in honor of Dr. Joseph Sanfilippo. Read the Press ReleaseUterine Aspiration of Pregnancy of Unknown Location
What CPT code would be most appropriate for a manual uterine aspiration for a pregnancy of unknown location? View the AnswerEligibility to bill for facility fee
We are planning to open a new fertility clinic and I was wondering about the eligibility to bill insurance companies for “facility fee” for egg retrievals. View the AnswerResection Adenomyoma
I have a patient with an adenomyoma of the uterine wall that requires surgical excision and uterine repair. View the AnswerRobotically Assisted Tubal Anastomosis
What is the correct CPT code for laparoscopic tubal anastomosis with robotic assistance? View the AnswerSurgery Coding
I took the ASRM coding course, and in that course, coding for bilateral neosalpingostomies was coded using only a dx of N70.11 (hydrosalpinx). View the AnswerTompkins Metroplasty
Is there a code for Tompkins Metroplasty? View the AnswerMultiple Laparoscopic Procedures
Is it appropriate to bill for medically indicated, multiple procedures when performing laparoscopies? View the AnswerOffice Hysteroscopy Billing
Do you all have a resource that details what all can be billed, or what all is bundled with the 58558 procedure when done in office? View the AnswerOvarian Drilling
Is there a CPT Code for "Ovarian Drilling"? View the AnswerOvariopexy
Is there a CPT code for Ovariopexy procedure only, via mini-laparotomy? View the AnswerExcision Ovarian Endometrioma
What code is used for a laparoscopic excision of endometriosis and an ovarian excision of endometrioma with bilateral ureterolysis is performed. View the AnswerHysteroscopic Tubal Cannulation Under Laparoscopic Guidance
How can one code for hysteroscopic transcervical fallopian tube cannulation under laparoscopic guidance? View the AnswerHysteroscopy Polyp Suspected
What ICD-10 code do you use if a diagnostic hysteroscopy is performed for the preoperative diagnosis of uterine polyp? View the AnswerHysteroscopy Recurrent Implantation Failure
What is the appropriate ICD-10 code for recurrent implantation failure? View the AnswerHysteroscopy Resection of Retained Products of Conception
What CPT is appropriate for a Hysteroscopy Resection of Retained Products of Conception? View the AnswerD&C Under Ultrasound Guidance
What are the CPT codes and ICD-10 codes for coding a surgical case for a patient with history of Stage B adenocarcinoma of the cervix ... View the AnswerDiagnostic Hysteroscopy
If the doctors do a hysteroscope #58555 in the office with a Endosee Scope, can I still use the same code even though it is in the office? View the AnswerCoding for Ovarian Drilling
Can you provide some information related to ovarian drilling that would assist non-physician administration (coders, billers)? View the AnswerCoding For Placement Of A Cervical Stitch
Physicians at our practice are placing a stitch and dilating the cervix after egg retrievals for those patients that have cervical stenosis. View the AnswerCycle Monitoring Fertility Preservation
If the patient is undergoing ultrasound tracking visits for fertility preservation, what I ICD-10 code do you use for the monitoring? View the AnswerC-Section Ectopic Pregnancy
I’m writing for advice for CPT advice for managing cesarean scar ectopic pregnancy without concurrent intrauterine pregnancy (ICD-10 O00.80). View the AnswerSRS Travel Scholar Award for Reproductive Surgery
The objective of the SRS Traveling Scholar Award is to provide for any trainee whose abstract submission focuses on reproductive surgery to expand their educational and networking experience. View the Award InformationSRS-SMRU Travel Scholar Award for Male Reproductive Surgery
The objective of the SRS-SMRU Traveling Scholars Award is for any trainee whose abstract submission focuses on male reproductive surgery to expand their educational and networking experience. View the Award InformationSRS In-Training Awards for Research
DeCherney-Nezhat REI Fellows Traveling Scholars Award in Reproductive Surgery
The objective of this award is to expand educational and networking opportunities for REI Fellows with a focus on reproductive surgery. View the Award InformationJournal Club Global: Moving leiomyoma research from bench to bedside
Postoperative adhesions in gynecologic surgery: a committee opinion (2019)
Postoperative adhesions are a natural consequence of surgical tissue trauma and healing and may result in infertility, pain, and bowel obstruction. View the Committee OpinionAmerican Society for Reproductive Medicine position statement on uterus transplantation: a committee opinion (2018)
Following the birth of the first child from a transplanted uterus in Gothenburg, Sweden, in 2014, other centers worldwide have produced scientific reports. View the Committee OpinionTopic Resources
IVF-assisted pregnancies constitute 2.5% of all births in 2022
In 2022, the number of babies born from IVF increased from 89,208 in 2021 to 91,771 in 2022. This means that 2.5% of births in the US are a result of ART.
View the Press ReleaseFertility and Sterility On Air - Unplugged: March 2024
Topics include: melatonin and implantation (4:38), whole-genome screening of embryos, and bioengineering assisted reproductive technology. Listen to the EpisodeASRM reacts to Alabama legislation
We are pleased that the legislation passed into law by the Alabama General Assembly will at least allow our members in the state to care for their patients.
View the Press ReleaseIVF at the SOTU: Fertility care expected to be major focus at State of the Union
Protecting access to IVF care is expected to be a major theme of the State of the Union on Thursday.
View the Press ReleaseASRM Responds to Proposed Alabama Legislation
We are proud of our Alabama members and their patients, who have been such incredible advocates working to motivate their legislators to protect IVF.
View the Press ReleaseSenate Budget Hearing is Well Timed Following Alabama IVF Ruling
ASRM statement regarding the Senate Budget Committee’s hearing entitled: No Rights to Speak of: The Economic Harms of Restricting Reproductive Freedom.
View the Press ReleaseASRM Responds to Senate’s Failure to Pass Access to Family Building Act
We are disappointed by the Senate’s failure to meet the moment and pass federal legislation protecting access to in vitro fertilization (IVF).
View the Press ReleaseASRM Condemns Profoundly Misguided and Dangerous Court Decision in Alabama
In LePage v Mobile Infirmary Clinic, the Alabama Supreme Court made a decision that flies in the face of medical reality and the needs of the citizens.
View the Press ReleasePrevention of moderate and severe ovarian hyperstimulation syndrome: a guideline (2023)
Ovarian hyperstimulation syndrome is a serious complication associatedwith assisted reproductive technology. View the guidelineASRM applauds introduction of Access to Family Building Act of 2024
ASRM is thrilled by the introduction of the Access to Family Building Act
View the Press ReleaseGuidance for coding limited or follow-up ultrasounds used during an IVF Cycle
I am a coder for a Reproductive Endocrinologist's office and am looking for some guidelines on limited or follow-up ultrasounds used during an IVF Cycle. View the AnswerMeasurements to report with ultrasound codes
Are there clear guidelines as to what measurements are required in order to bill for each type of ultrasound? VIew the AnswerBilling for cryopreservation procedures on different days
I understand that if cryopreservation of oocytes is performed on two separate dates of service, each date of service was billable. View the AnswerBilling IVF lab work
We typically bill our IVF Lab work under the rendering provider who performs the VOR. Who should be the supervising provider for embryology billing? View the AnswerEstradiol Free versus Total
Should patients with fertility issues be billing Estradiol Free (82681) instead of Estradiol Total (82670)? View the AnswerIVF coverage denied for Z31.83 diagnosis code
My wife and I have been seeking IVF treatment and coverage was added for infertility treatment (up to $25,000) but our insurer keeps denying it. View the AnswerCycle coordination fees and 99499, S4042
I reviewed cycle coordination fees, but see that there is no specific code for cycle management. View the AnswerSupervising provider for embryology billing
We typically bill our IVF Lab work under the rendering provider who performs the VOR. Who should be the supervising provider for embryology billing? View the AnswerThe International Glossary on Infertility and Fertility Care, 2017†‡§ (2017)
Terms and definitions currently used infertility care, infertility and medically assisted reproduction (MAR) can have different meanings that are dependent upon the setting, their usage in research or clinical interventions, or among diverse populations.View the Committee Joint Guideline
Journal Club Global - Revisiting the STAR trial: The Fellows debate PGT-A
We are excited to host a debate covering the pros and cons of PGT-A and how new technologies should be validated before clinical implementation. View the VideoInformed consent in assisted reproduction: an Ethics Committee opinion (2023)
Informed consent is a process in which the patient is supported in developing an understanding of medical options. View the Ethics Committee OpinionUnlisted Fertility Treatment CPT Code
Can you please refer me to an unlisted management CPT code for fertility treatment? View the AnswerZ Codes Vs. Procedure Codes For Fertility Preservation Counseling
I am trying to understand better when to use the procreative management code vs the fertility preservation counseling and procedure codes. View the AnswerPregnancy Of Unknown Location
What is the most appropriate ICD-10 code for pregnancy of unknown location (not an ectopic pregnancy)? View the AnswerPregnancy Ultrasound
Our practice does routine ultrasounds (sac check- 76817) at the end of an IVF cycle and bill with a diagnosis code O09.081, pregnancy resulting from ART. View the AnswerIUI Same Gender
When managing an IUI or IVF cycle for a female same sex couple or a patient that has no exposure to sperm, what ICD 10 diagnosis should be used? View the AnswerIVF Case Rates
What ICD-10 codes apply to case rates? View the AnswerLimited Monitoring Ultrasound
What is the appropriate code to use for a limited follow-up follicular transvaginal ultrasound? View the AnswerLimited Transvaginal Ultrasound
One of our clients received information that a repeat limited transvaginal ultrasound should be billed with a limited pelvic ultrasound code (76857). View the AnswerMonitoring E&M
Our group would like to know if others are billing an evaluation and management code for ultrasound and blood draw visits? View the AnswerMonitoring FET
What is the correct diagnosis code to use on the follicle ultrasound (76857) for a patient who is undergoing frozen embryo transfer (FET)? View the AnswerMonitoring Ovulation Induction By Nurses
We are considering the use of CPT code 99211 for encounters during cycle management as part of ovulation induction. View the AnswerNon-REI Board Certified MD Performing REI Procedures
My boss has a few follow up questions about a non-REI board certified MD performing REI procedures. View the AnswerIn Vitro Maturation
Have CPT codes been established for maturation in vitro? View the AnswerEmbryo Storage Fees For Multiple Cycles
We bill embryo storage 89342 for a year's storage. View the AnswerEndometrial Receptivity Analysis
Our physicians are going to start doing an Endometrial Receptivity Analysis. Do you know the appropriate CPT code that should be used?View the Answer