
Multiple gestation associated with infertility therapy: a committee opinion (2021)
The goal of infertility treatment is for each patient to have one healthy child at a time. The challenges associated with achieving that goal differ by treatment and clinical context. In ovulation induction (OI), which is used in cases of oligo- or anovulation, ovulation of more than the targeted single oocyte occasionally results. In ovarian stimulation (OS), which is used in ovulatory women with other infertility diagnoses, implantation of more than one embryo may follow the fertilization of oocytes from supernumerary follicles. With assisted reproductive technologies (ART), multiple embryos may be transferred, or monozygotic twinning can occur. Regardless of which treatment is performed, the objective is the same: to maximize the probability of pregnancy while minimizing the risk of a multiple gestation. The objectives of this committee opinion include the following:
- Review the incidence, recent trends, and modes of conception associated with multiple gestations in the US.
- Consider the different factors associated with the increased risk for multiple pregnancies in OI, OS, and ART.
- Discuss the complications and economic impact of multiple pregnancies.
- Summarize current and emerging strategies aimed at limiting the risk of multiple gestations associated with treatments for infertility.
MULTIPLE BIRTHS IN THE US
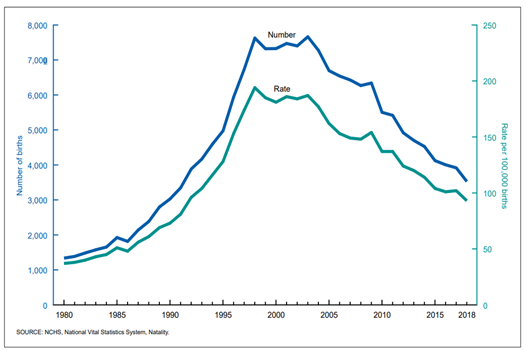
The incidence of multiple births in the US has risen since 1980, which is considered as the reference year for estimating the relative contributions of different infertility treatments to the multiple birth rate. At that time, clinical practice in the US did not include in vitro fertilization (IVF), and the use of exogenous gonadotropins for OI and OS was limited (1). From 1980 to 2014, the twin birth rate in the US increased from 1 in 53 births to 1 in 29 births, a 79% relative increase (2). This was the result of a 2% annual increase in twin rates from 1980–2003 and a 1% annual increase from 2003– 2014 (Fig. 1). After more than 3 decades of rising twin birth rates, there was a 1% reduction per year from 2014– 2018, resulting in a 4% overall decrease in the twin rate (2).Figure 1
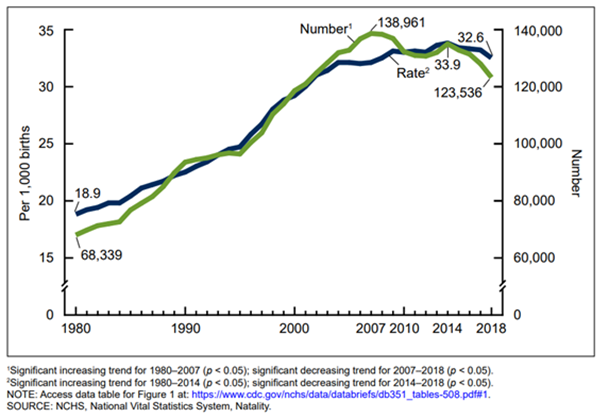
Figure 2
Accurate estimates of the relative proportions of multiple births attributable to OI/OS are difficult to determine, as these cycles are not currently captured in a national registry. The estimated contribution of OI/OS cycles was derived from the total number of multiple births nationally minus the sum of the ART contribution and the estimated number from natural conception. Even with these caveats, there is consensus that most of the twin births result from natural conception (60%), with OI/OS and ART treatments accounting proportionally for the remainder (OI/OS: range 21–32%; ART: range 8–16%) (1, 5–7). Although there is agreement that 20% of high-order multiple gestations result from natural conception (1, 5–8), allocation of the remainder to OI/OS vs. ART varies widely (OI/OS: range 39–67%; ART: range 13–44%) (1, 5, 7). Although naturally conceived twins account for most of all multiple births, the incidence of twins among births resulting specifically from infertility treatments is more than 20 times greater than that for births resulting from natural conception, and that of high-order multiple gestation is more than 100 times higher (6). Therefore, attention must remain focused on efforts to decrease the risk of multiple gestation associated with infertility treatment.
RISK FACTORS FOR THE OCCURRENCE OF MULTIPLE GESTATIONS
In naturally conceived multiple gestation, the prevalence of dizygotic twinning varies with ethnicity (1.3/1,000 in Japan, 8/1,000 in the US and Europe, and 50/1,000 in Nigeria) (9, 10). Dizygotic twinning is also associated with increased maternal age, greater parity, and a maternal family history of twinning (9, 11, 12). In contrast, the rate of monozygotic twinning is relatively constant (4/1,000 live births) (13), regardless of maternal age, race, or parity (14), although genetic predisposition may have some influence (15).Multiple follicular development is the dominant risk factor for dizygotic twinning and high-order multiple gestation in OI and OS cycles (16). In ART treatment, the main risk factor for dizygotic and high-order multiple pregnancies is the transfer of more than one embryo (17, 18). The risk of monozygotic twinning may be increased by approximately twofold in ART cycles, and the contributions of specific ART techniques have been investigated (14, 19, 20). Data from the National ART Surveillance System demonstrated that assisted hatching was associated with an increased risk of monozygotic twins (21). This was consistent with the results of a meta-analysis of 16 studies and nearly 300,000 ART cycles (22), which found mixed results for monozygotic twinning with intracytoplasmic sperm injection compared to conventional insemination. A number of studies have concluded that the risk of monozygotic twinning is increased when culture is extended to the blastocyst stage (15, 21, 22). One report suggested that the risk may be related to the composition of culture media (23).
COMPLICATIONS OF MULTIPLE GESTATIONS
Multiple gestation increases maternal morbidity and fetal and neonatal morbidity and mortality. The most important maternal complications associated with multiple gestation are preeclampsia, gestational diabetes, and preterm labor and delivery (Table 1) (24–31). Other complications of multiple gestation include cholestasis, dermatoses, excess weight gain, anemia, hyperemesis gravidarum, and exacerbation of pregnancy-associated gastrointestinal symptoms (reflux, constipation) (31–34). Chronic back pain, intermittent dyspnea, postpartum laxity of the abdominal wall, and umbilical hernias also occur frequently. Most of the excess perinatal morbidity and mortality associated with multiple gestations is directly related to the consequences of preterm birth (Table 1).Table 1. Incidence (%) of Major Maternal Complications in Multiple Pregnancies (24-29).
| Singleton | Twin | Triplet | Quadruplets | |
| Pre-eclampsia | 6 | 10-12 | 25-60 | >60 |
| Gestational diabetes | 3 | 5-8 | 7 | >10 |
| Pre-term labor | 15 | 40 | 75 | >95 |
| Delivery at <37 weeks | 10 | 50 | 92 | >95 |
| Delivery at <32 weeks | 2 | 8 | 26 | >95 |
Table 2. Major Perinatal Morbidity and Mortality Outcomes in Multiple Pregnancies (, 31, 35, 39).
| Singleton | Twin | Triplet | |
| Prospective risk of fetal death (%)* | 0.03 | 0.09 | 0.14 |
| Getational diabetes (%) | 0.06 | .31 | 1.38 |
| Neonates <2500g (%) | 6.2 | 53.2 | 93.2 |
| Neonates <1500g (%) | 1.2 | 10.5 | 37.5 |
| Average gestational age (weeks) | 39.1 | 35.3 | 32.2 |
| Average birth weight (g) | 3358 | 2347 | 1687 |
| *Prospective risk of fetal death between 24 and 43 weeks gestation in a singleton pregnancy, 41 weeks in a twin pregnancy, and 38 weeks in a triplet pregnancy; prospective risk calculated as a proportion of all fetuses still present at a given gestational age because gestational age varies by the number of fetuses. | |||
Table 3. Neonatal Outcome in Singleton and Vanishing Twin Gestations (Pinborg2005).
| Singleton | Surviving twin | |
| Delivery at <37 weeks (%) | 9.0 | 13.2 |
| Delivery at <32 weeks (%) | 1.3 | 3.8 |
| Neonates <2500g (%) | 6.3 | 11.7 |
| Neonates <1500g (%) | 1.5 | 4.1 |
| *P<0.001 for comparison between singleton and surviving twin for each outcome | ||
Placenta previa, vasa previa, and abruptio placenta also occur more frequently in multiple gestations (47, 48), with abruptio placenta being the most common. Postpartum hemorrhage also complicates approximately 12% of multifetal deliveries (33). The risks associated with multiple gestation include the consequences of preterm birth (cerebral palsy, retinopathy, and bronchopulmonary dysplasia) and those of fetal growth restriction (polycythemia, hypoglycemia, and necrotizing enterocolitis). To what extent multiple gestation itself may affect neurobehavioral development in the absence of these complications remains unclear.
ECONOMIC CONSIDERATIONS FOR MULTIPLE GESTATIONS
The economic costs relating to excess perinatal and maternal morbidity and mortality associated with multiple gestations resulting from OI, OS, and ART are substantial and include both the immediate costs of maternal hospitalization and neonatal intensive care and the lifetime costs of care for chronic illness, rehabilitation, and special education. The immediate costs associated with multiple gestation can be estimated from hospital charges, whereas the lifetime costs are more difficult to determine–although they have been estimated in several studies from Europe, Canada, and the US (49). The medical expenses associated with twin gestation are approximately 5 times greater than those associated with singleton pregnancies, and pregnancies with delivery of high-order multiples cost nearly 20 times more (50). Even after birth, the hospital costs until the age of 5 years are significantly higher for multiples compared to that for singletons born after IVF (51). Aside from the medical costs associated with obstetric and neonatal management of multiple gestation, raising twins is likely to be more expensive for a family compared to the cost of raising 2 singletons. The US Department of Agriculture estimates that the cost for a middle-income family to raise a set of twins ($499,680) is more than double the cost of raising a singleton ($233,610) (52).FACTORS CONTRIBUTING TO THE INCREASED RISK OF MULTIPLE GESTATION ASSOCIATED WITH TREATMENTS FOR INFERTILITY
Several factors contribute to the increased incidence of multiple gestation resulting from treatments for infertility. An increased sense of urgency leads many couples with infertility to pursue more aggressive treatments involving the use of exogenous gonadotropins or to accept the risks associated with the transfer of greater numbers of embryos in IVF cycles. Although multiple birth rates are lower in states having comprehensive health care insurance mandates that include IVF, it is unclear whether the differences relate to more conservative embryo transfer practices or to the characteristics of patient populations having greater access to such treatment (53–55). Inadequacy or absence of health insurance coverage for IVF may encourage some to pursue OS as a less costly alternative. Another strategy when health insurance coverage is inadequate is to increase the number of embryos transferred in the one or few IVF cycles that limited resources will allow (56).In 1998, SART and American Society for Reproductive Medicine published the first practice guidance documents for the maximum numbers of embryos to transfer in IVF cycles according to maternal age and other prognostic factors. Recommendations were adjusted downward in subsequent updates issued in 2004, 2006, 2008, 2009, 2013, and 2017, (69). as IVF success rates and multiple gestation increased (53, 57–61). In these documents, multiple embryo transfer was still considered acceptable in all but the most favorable patients <35 years of age. The updated committee opinion for the maximum numbers of embryos to transfer published in 2017 was significantly different (61). Based on registry data showing that clinics performing high rates of single embryo transfer (SET) in woman <38 years of age have reduced multiple gestation rates without a negative impact on cumulative live birth rates, and single-blastocyst transfer was recommended in all patients younger than 38 years of age with a favorable prognosis (61, 62). With the increasing use of blastocyst-stage biopsy for preimplantation genetic testing for aneuploidy (PGT-A), the 2017 document included, for the first time, guidance on the transfer of euploid embryos. Single embryo transfer was recommended for euploid embryos regardless of maternal age or prognosis. The decline in IVF-related and overall US high-order multiple gestation births has temporally followed the release of each new guidance document with a continued decline in triplet births, accounting for only 0.2% of ART deliveries in 2018 (63, 64).
Single embryo transfer rates remained below 10% for all ages through 2009. With the increasing use of extended embryo culture and blastocyst vitrification, there was a dramatic increase in SET. In 2018, 67.3% of all transfers were SETs (65). Due to the change in transfer practices, the twin rate has recently dramatically declined to <10% of all IVF births (66).
Gestational carriers (GCs) are being increasingly utilized in IVF cycles as they present an alternative to adoption and allow the intended parent(s) to potentially maintain a genetic link with their offspring. In the US, GC use in IVF cycles has increased from 1%–3.5% of all IVF cycles (67–69). There is also increasing utilization of GCs in the US by individuals from foreign nations where GC use is much more restricted (67). Due to the high cost of GC IVF cycles, many intended parents are tempted to transfer multiple embryos to increase their odds of live birth. This was confirmed by a survey of Centers for Disease Control and Prevention ART data, in which >30,000 GC IVF cycles were reviewed, of which 78.6% had >1 embryo transferred (68). Unsurprisingly, this same study also reported that of 13,380 deliveries, 34% were twins, and 2% were high-order multiples, which is significantly higher than the incidence of twins and high-order multiples in naturally conceived pregnancies (69). Similarly, in a more recent analysis of oocyte-donor recipient GC IVF cycles from 2014–2016 SART data, of 4,776 IVF cycles analyzed, 48.7% involved transfer of >1 blastocyst with an overall mean of 1.5 ± 0.5 embryos transferred. Transfer of >1 blastocyst in these patients resulted in multiple pregnancy rates between 41.5% and 45.6% (70).
Given the significant maternal and neonatal risks of multiple gestation that we have already summarized, it is crucial to prioritize the health and safety of these altruistic women and preserve the invaluable service they provide by promoting the use of SET.
STRATEGIES FOR LIMITING THE RISK OF MULTIPLE GESTATION IN ART
The most direct way to limit the risk of multiple gestation from ART is to transfer a single embryo. Transferring multiple embryos results in higher overall live birth rates per transfer but also incurs an increased risk of multiple gestation with increased obstetric and neonatal complications (71). Methods for embryo selection have evolved using technologies but still do not perfectly predict the single embryo having the greatest implantation and developmental potential. It is also difficult to predict the likelihood of pregnancy and of multiple gestation on the basis of patient characteristics. Therefore, efforts to reduce multiple gestation have focused on increasing utilization of SET.Many factors influence the application of elective SET (eSET), a few of which are mentioned below:
- The desire to achieve a higher per transfer pregnancy rate.
- The education of both clinicians and patients on the health and wider societal benefits of eSET.
- The availability of health insurance coverage for IVF sufficient to permit repeated attempts at fresh and frozen embryo transfer.
- The economic pressure on patients restricting the number of ART cycles that they can attempt.
- Other socioeconomic, cultural, and religious factors.
Embryo transfer policies vary among countries and range from strict government regulations to more flexible professional guidelines. In the US, ART professionals have developed prognosis-dependent guidelines that allow for greater individualization of patient care while still limiting the risk for multiple gestation (64). Such practice guidelines ultimately leave the decision to physicians and their patients (Table 4) (53) but recognize that patients having the best prognosis should have fewer embryos transferred.
Table 4: Recommendations for limiting the number of embryos to transfer (53)
| Prognosis | Age (years) | ||||
| <35 | 35-37 | 38-40 | 41-42 | ||
| Cleavage stage embryos | |||||
| Euploid(a) | 1 | 1 | 1 | 1 | |
| Othr favorable (b) | 1 | 1 | <3 | <5 | |
| Embryos not euploid (a) or favorable (b) | <2 | <3 | <4 | <5 | |
| Balstocysts | |||||
| Euploid(a) | 1 | 1 | 1 | 1 | |
| Othr favorable (b) | 1 | 1 | <2 | <3 | |
| Embryos not euploid (a) or favorable (b) | <2 | <2 | <3 | <3 | |
| (a) Demonstrated euploid embryos, best prognosis (b) Other Favorable = Any ONE of these criteria: Fresh cycle: expectation of 1 or more high-quality embryos available for cryopreservation or previous live birth after an IVF cycle; FET cycle: availability of vitrified day-5 or day-6 blastocysts, euploid embryos, 1st FET cycle, or previous live birth after an IVF cycle. **Please note that justification for transferring additional embryos beyond recommended limits should be clearly documented in the patient’s medical record. |
|||||
- Expectation of one or more high-quality embryos available for cryopreservation.
- Previous live birth after an IVF cycle.
- For frozen embryo transfers (FETs): vitrified blastocysts, euploid embryos, first FET cycle, previous live birth from IVF.
Single Embryo Transfer
Increasing the likelihood of live birth from each transfer event could theoretically increase the willingness of patients and providers to use SET, both in the initial embryo transfer and in subsequent transfer cycles. Strategies to improve live birth have primarily focused on maximizing embryo selection and endometrial synchrony. These strategies include PGT-A, freezing only embryo transfer cycles, endometrial synchrony testing, and time lapse imaging and other noninvasive embryo testing strategies. There is currently a lack of robust and consistent evidence that these strategies improve the chances of achieving a live birth. Furthermore, while strategies to improve live birth are aimed at improving the live-birth success of each embryo transfer, they are not required to reduce multiple gestation. Performing SET without additional embryo or endometrial testing is sufficient to reduce the multiple gestation rate down to the background 1–2% risk of monozygotic twins in ART (74, 77, 78). Single embryo transfer, regardless of additional testing, should be considered the gold standard to reduce multiple gestation. Given the lack of robust evidence or conflicting evidence for many of these tests to improve clinical outcomes, they are currently not routinely recommended as a strategy to increase SET.Extended Culture–Single Blastocyst Transfer
The effectiveness of SET may be maximized by transfer of a blastocyst rather than a cleavage-stage embryo. In one program in the US, implementation of a policy to transfer a single blastocyst, combined with an educational program relating specifically to the potential risks and consequences of multiple births, resulted in a substantial decrease in the average number of embryos transferred and in the incidence of multiple gestation (from 35%–19%), while overall pregnancy rates were maintained (79). This result was replicated in another US center where introduction of a single blastocyst transfer policy in good-prognosis patients maintained clinical pregnancy at 63% but reduced twin gestation from 44%–15% (80).A randomized trial comparing single cleavage-stage embryo transfer vs. single blastocyst-stage embryo transfer found that the blastocyst-stage group had a significantly higher rate of live birth (32.0% vs. 21.6%, relative risk [RR] 1.48 [95%CI 1.04–2.11]) (81). This difference may be partially attributable to a higher rate of pregnancy loss in the first trimester in the cleavage-stage group than in the blastocyst-stage group, although this difference was not significant (33.9% vs. 19.2%). There were 2 monozygotic twin pregnancies, both occurring in the cleavage-stage transfer group (81)
A small, randomized trial from a single center did not show a significant difference between the transfer of 1 vs. 2 blastocysts, with ongoing pregnancy rates of 60.9% and 76%, respectively, and twin rates of 0% and 47.4%, respectively (74). The study did not include a discussion of how the sample size was chosen. Since it included only 48 patients, SET could have been as much as 41% inferior to DET (95% risk difference). While intriguing, these 2 trials did not significantly change clinical practice, as transfer of 2 blastocysts remained the predominant practice throughout the early 2000s. However, there are several theoretical concerns with blastocyst transfer, including an increased incidence of monozygotic twinning with one large registry study finding a 2% risk among cleavage-stage transfers and a 3.4% risk among blastocyst transfers (OR 1.7, 95%CI 1.05–2.76). Elective SET was also an independent risk factor for monozygotic twinning. There also are fewer embryos available for cryopreservation (81) after blastocyst transfer, possibly limiting cumulative pregnancy rates. Based on animal data (82), there is theoretical concern that extended culture to the blastocyst stage may be associated with epigenetic changes in the embryo (83). While these theoretical concerns exist, the vast majority of data suggest that blastocyst-stage transfer is safe and effective.
Preimplantation Genetic Testing for Aneuploidy
While originally developed to improve outcomes for poor prognosis IVF patients (prior failed cycles, advanced age, recurrent pregnancy loss), in recent years, PGT-A has been used as a strategy to enhance selection for eSET. In a retrospective study, Forman et al. (84) found that single euploid blastocysts resulted in a 55% ongoing pregnancy rate compared to 41.8% among untested blastocysts. A randomized, noninferiority trial by the same group showed that euploid eSET resulted in similar live birth rates as that of the transfer of 2 untested blastocysts, with a significantly lower risk of multiple gestation. Among 175 randomized patients up to age 42 years with normal ovarian reserve, there was a 60.7% ongoing pregnancy rate after euploid eSET vs. 65.1% after untested DET (85). Follow-up of randomized patients including a subsequent transfer for those who did not deliver on their first attempt, demonstrated improved obstetric outcomes in the eSET group (86). While these studies used a real-time polymerase chain reaction for PGT-A, next generation sequencing has become more widely used. The STAR Trial was an RCT comparing FET of a single euploid blastocyst testing with next generation sequencing to SET of a blastocyst selected by morphology. Embryos with a mosaic result on PGT-A were excluded from transfer. Overall, the study did not show improved ongoing pregnancy rates after PGT-A(87). The data on PGT-A are insufficient to recommend its
routine use for the purpose of increasing SET.
STRATEGIES FOR LIMITING THE RISK OF MULTIPLE GESTATION IN OVULATION INDUCTION AND OVARIAN STIMULATION TREATMENTS
The historic and putative goals of OI and OS differ significantly depending on the clinical context. The ideal goal of OI in oligo-ovulatory or anovulatory women should be ovulation of a single mature oocyte. In contrast, the goal of OS in ovulatory women is to cautiously manage multi-follicular recruitment in an effort to increase cycle fecundity, while also minimizing the increased risk of multiple gestation.Anovulatory Infertility
It is imperative to tailor a patient’s stimulation regimen to their specific clinical circumstance and need. There are multiple OS agents that can be used, varying from oral agents to gonadotropin injections. For anovulatory women, such as those with polycystic ovary syndrome, the most recent Cochrane review showed that letrozole compared to clomiphene citrate (CC) increased live birth rates (OR 1.68;95% CI 1.42– 1.99) without increasing the multiple pregnancy rate (1.7% with CC vs 1.3% with letrozole; OR 0.69%;95% CI 0.41–1.16) (88). A meta-analysis of 57 RCTs with 8,082 women also confirmed that letrozole resulted in significantly higher live birth rates compared to clomiphene and with a lower incidence of multiple gestation compared to gonadotropins, which had the greatest risk of multiple gestation (89). However, if ovulation is not achieved using oral agents, low-dose exogenous gonadotropins are acceptable to use for OI cycles with a strict cancellation policy. It is recommended to start at a low dose of 37.5–75 IU a day, with slow increases of dosing to achieve mono-follicular development. Further, cycle cancellation is strongly recommended for patients with >2 follicles R16 mm or if there are R3 intermediate sized follicles to reduce the risk of multiple gestation and ovarian hyperstimulation syndrome (90).Unexplained Infertility
It is not recommended for most couples with unexplained infertility to undergo OS with gonadotropins. A recent systematic review and meta-analysis of 8 RCTs (2,989 women) showed no increase in live birth rates with gonadotrophins as compared to oral agents if gonadotropins were used in low doses or with a strict cancellation policy (91). However, if gonadotrophins were used in higher doses or without a strict cancellation policy, there was an increased pregnancy rate (RR 1.09) but with a concurrent increase in multiple gestations (RR 1.20 for higher doses and 1.15 for lax cancellation policy). Another meta-analysis had similar findings, indicating that gonadotropins had the highest live birth and ongoing pregnancy rates, but at the expense of a higher risk of multiple gestation (92). Considering all the associated maternal and neonatal complications with multiples, this increase in the rates of pregnancy and live birth does not ameliorate the negative outcomes of a similar increase in multiple gestation. Based on these findings, it is prudent to offer a course of OS with oral medications and intrauterine insemination (IUI) followed by IVF for those not successful (93, 94).Ovulatory Women Undergoing Donor Insemination
Donor insemination is utilized in ovulatory women who are infertile due to being same sex couples, single females, heterosexual couples with azoospermia, and other clinical scenarios. When ovulatory women are using donor sperm, both natural cycle and OS are management options. A recent retrospective cohort study (76,643 IUI cycles) compared natural cycle vs. OS in ovulatory women using donor sperm. There was a <1% increase in ongoing pregnancies with oral medications compared to the natural cycle, but ongoing multiple gestations increased from 2.4%–10.8%. Based on limited data, natural cycle IUI should be considered as the first-line treatment for ovulatory women who are using donor sperm insemination (95).Mitigating the Risk of Multiples
In a multicenter RCT involving 1,220 OS cycles in which human chorionic gonadotropin was withheld when the E2 level exceeded 3,000 pg/mL or when >4 follicles >18 mm in diameter were observed, the multiple pregnancy rate was very high at 31%, with 6% of pregnancies being triplets (96). In another trial involving 449 OS cycles in which human chorionic gonadotropin was withheld if >6 follicles >14–15 mm in size were observed, the overall multiple pregnancy rate was 23.5%, of which 92% were twins, and 8% were high-order multiples (97). These data clearly demonstrate that lax cancellation policies during OS result in a significant risk of both twin and high-order multiple gestation. Conversely, another study showed that when cycles were cancelled if >3 follicles R14 mm developed, multiple gestation could be limited to only 2% (98). Evidence derived from experience in ART cycles indicates that follicles as small as 10 mm in diameter may yield mature and fertilizable oocytes (99).Specifically looking at age and number of follicles during OI or OS, a retrospective cohort study with 50,473 OI/OS and IUI cycles concluded there was a marked increased risk of multiple gestation if proceeding with IUI in women younger than age 40 years with >2 follicles R14 mm (100). In addition, there was no improved chance of a singleton clinical pregnancy and minimal increase in overall pregnancy with >2 follicles. When comparing 1 mature follicle vs. 5 at time of IUI in women <38 years of age, clinical pregnancy rates ranged from 14.6%–21.9% but with an increase in multiple gestation risk from 4%–31.8% with 1 vs 5 follicles. Similar findings were noted in the 38–40 years of age group. Conversely, in women > 40 years of age, up to 3 follicles increased the odds of pregnancy (aOR 5.76 [95%CI 0.69– 48.25]) while keeping the rate of multiple gestation per pregnancy at <8%. Subanalysis demonstrated that with increasing follicle number, the increased risk of multiple gestation and minimal benefit in pregnancy persisted in patients with both anovulation and unexplained infertility
(100). This challenges the historic approach of trying to develop more follicles in ovulatory patients with infertility to increase the chance of pregnancy. Though this model outlined by the investigators serves as a helpful clinical counseling tool, it is not an established predictor given that the studied population represents a heterogeneous group with a wide range of prognosis for both fecundity and multiple gestations.
When gonadotropins are used for treatments outside of ART, low-dose gonadotropins (37.5–75 IU per day) should be utilized to minimize the risk of multiple gestation. However, the above evidence demonstrates that the benefit of low-dose gonadotropin use is primarily in the setting of anovulatory patients who do not respond to oral medications. In the setting of ovulatory patients, the data demonstrate that gonadotropin use increases pregnancy only when used at high enough doses that the risk of multiple gestation is also increased. When gonadotropins are used on ovulatory women at low doses with a strict cancellation policy, live birth is not increased, and cost is increased (101).
The clinical utility of preovulatory ultrasound-guided aspiration of excess follicles for reducing the risk of multiple gestation in OI and SO has been examined (102–104). In 2 studies, aspiration was performed when >3 follicles having a mean diameter of >14 mm were observed, leaving the 3 largest follicles undisturbed (93, 102). The multiple gestation rate was approximately 10%, and the overall pregnancy rates ranged between 20% and 25%. In the third study, in which aspiration was performed when >3 follicles measuring >15 mm in mean diameter were observed, and all follicles <15 mm in size were aspirated (105), the pregnancy rate was 26.9% per cycle, and no multiple pregnancies occurred. Taken together, these data suggest that additional studies are warranted to better define the optimal criteria and methods for aspiration and the overall cost-effectiveness of the strategy. Overall, regardless of which medication or stimulation regimen is used, it may not be possible to entirely eliminate the risk of multiple gestation associated with OI or OS. Follicle aspiration to reduce the risk of multiple gestation in this setting should only be considered as a risk mitigation strategy for unanticipated over response to medication, not as a standard approach for non-ART treatments.
MULTIFETAL PREGNANCY REDUCTION
High-order multifetal gestation must be regarded as an adverse outcome of treatment for infertility. The risk for adverse perinatal and maternal outcomes increases progressively with the number of fetuses (106, 107) Patients with high-order multiple gestations must choose one of 3 options: continuing the pregnancy, accepting all of the risks previously described; terminating the pregnancy; or multifetal pregnancy reduction (MFPR) to reduce the number of fetuses and the associated risks of maternal and perinatal morbidity and mortality (106, 108, 109). Multifetal pregnancy reduction decreases the risks associated with preterm delivery (109–111), whether in quadruplets or above (110), trichorionic triplets reduced either to twins (112) or to singletons (106, 113, 114), or after reduction of a monochorionic pair in a triplet pregnancy (115). However, because MFPR can present patients with a profound ethical dilemma and cause significant psychologic trauma (107, 116), thorough counseling must be provided (105). A study of 91 patients indicated that despite feelings of loss and guilt for at least a year (117), most (93%) would make the same decision for MFPR if faced with a similar situation in the future (118). Patients who describe themselves as ‘‘pro-choice’’ are more likely to consider MFPR than those who do not, and their views do not change after having an embryo transfer (119). The primary risks of MFPR are pregnancy loss and preterm birth. However, as experience with the procedure has grown, the incidence of pregnancy loss and premature birth has further declined (109, 110, 113). It is recommended that MFPR should be performed only in specialized centers with fetal medicine practitioners experienced in the procedure (109, 110).Literature on the benefits of MFPR is limited by a lack of randomized trials assessing efficacy (owing to obvious ethical considerations) and a paucity of meta-analyses. Consequently, a systematic review concluded that the data are insufficient to recommend a general policy of MFPR for women with a high-order multiple pregnancy (120). Nevertheless, several analyses have shown that MFPR does appear to benefit quadruplet and higher-order pregnancies wherein the procedure clearly prolongs the length of gestation for the remaining fetuses (109, 110, 120). Moreover, the results of one meta-analysis of 11 nonrandomized studies of triplet pregnancies of varying quality (109) showed that the pregnancy loss rate at <24 weeks was similar in triplet pregnancies reduced to twins and in unreduced triplets (7% vs. 7.4%; OR 0.95, 95% CI 0.66–1.4). However, the preterm delivery rate at <28 weeks was significantly lower in the reduced triplets (2.9% vs. 9.8%; OR 0.30, 95% CI 0.18–0.5), as was the rate of preterm delivery at <32 weeks (8.9% vs. 25.1%; OR 0.36,
95% CI, 0.27–0.46) (109).
Therefore, available evidence indicates that MFPR appears to be associated with a reduced risk of prematurity, although the true benefit of this intervention is difficult to enumerate owing to potential bias in interpreting the data.
SUMMARY
- The goal of infertility treatment is for each patient to have one healthy child at a time. The challenges associated with achieving that goal differ by treatment and clinical context.
- The incidence of multiple births in the US has risen since 1980, likely driven almost entirely by infertility treatments.
- Subsequently, the percentage of high-order multiple gestations in the US has decreased since 1998, and twin gestation has decreased since 2014.
- A desire to achieve pregnancy expeditiously with fertility treatment must be balanced against the substantial family, medical, social, and economic consequences of multiple gestations.
- It is recommended that intentional strategies to reduce multiple gestation be employed in all infertility treatments, as multiple gestations are associated with major maternal and fetal risks.
- It is recommended that cycle cancellation should be considered if >2 follicles R16 mm develop or >3 follicles R14 mm develop in non-ART treatments in women <40 years of age. It should be noted that OI and OS result in
- more twin gestation than do ART treatments. Most of the high-order multiple gestations result from OI and OS rather than from ART or natural conception.
- It is recommended that in women with anovulatory infertility who require gonadotropins, the lowest dose possible be used to induce ovulation of a single follicle. Starting doses of 37.5–75 IU are recommended with small incremental increases as needed on the basis of ovarian response.
- It is not recommended to use gonadotropins for ovulatory women utilizing timed intercourse or IUI.
- It is recommended to use SET in all good-prognosis ART cycles. Elective SET is the most effective strategy for reducing the risk of multiple pregnancy with ART.
- Single embryo transfer should be strongly recommended in all GC cycles, given the health risks associated with multiple gestation for the GC. At a minimum, it is recommended to follow age-related limits on the number of embryos to transfer in GC cycles, on the basis of age of the oocytes from the intended parent or oocyte donor.
- It is not recommended to use alternate embryo and endometrial testing strategies purely for the purpose of
- increasing SET, as alternate strategies have not been proven to improve live birth or reduce multiple gestation compared to SET in good-prognosis patients.
- It is recommended to use patient educational strategies regarding the risks of multiple gestation to increase acceptance of SET and safe OS.
CONCLUSIONS
- Current efforts should continue to focus on reducing the overall incidence of multiple pregnancies, with increasing priority for reducing the twin rate.
- Greater efforts are needed to reduce the multiple gestation risk in non-ART infertility treatments, which estimates suggest are the greatest contribution to iatrogenic multiple gestation.
- Further research is needed on alternate methods of testing embryo and endometrial capacity to optimize live birth before they become routinely recommended.
- Physicians should counsel their patients carefully on the risks and benefits of eSET.
- Single embryo transfer should be utilized for all good-prognosis patients.
Acknowledgments: This report was developed under the direction of the Practice Committees of the American Society for Reproductive Medicine, the Society for Reproductive Endocrinology and Infertility, and the Quality Assurance Committee for the Society of Assisted Reproductive Technologies as a service to its members and other practicing clinicians. Although this document reflects appropriate management of a problem encountered in the practice of reproductive medicine, it is not intended to be the only approved standard of practice or to dictate an exclusive course of treatment. Other plans of management may be appropriate, considering the needs of the individual patient, available resources, and institutional or clinical practice limitations. The Practice Committees, the Quality Assurance Committee, and the Board of Directors of the American Society for Reproductive Medicine have approved this report. This document was reviewed by ASRM members, and their input was considered in the preparation of the final document.
The following members of the ASRM Practice Committee participated in the development of this document: Alan Penzias, M.D.; Kristin Bendikson, M.D.; Marcelle Cedars, M.D.; Tommaso Falcone, M.D.; Karl Hansen, M.D., Ph.D.; Micah Hill, D.O.; Sangita Jindal, Ph.D.; Suleena Kalra, M.D., M.S.C.E.; Jennifer Mersereau, M.D.; Richard Reindollar, M.D.; Chevis N Shannon, D.P.H., M.P.H., M.B.A.; Anne Steiner, M.D., M.P.H.: Cigdem Tanrikut, M.D.; Belinda Yauger, M.D. The Practice Committee acknowledges the special contribution of Task Force members Micah J Hill, D.O. (Chair), Erica Lowden, M.D., Eric Forman, M.D., Daniel Grow, M.D., and Mae Healy, D.O. in the preparation of this document. All Committee members disclosed commercial and financial relationships with manufacturers or distributors of goods or services used to treat patients. Members of the Committee who were found to have conflicts of interest based on the relationships disclosed did not participate in the discussion or development of this document.
REFERENCES
- Jones HW JR. Iatrogenic multiple births: a 2003 checkup. Fertil Steril 2007; 87:453–5.
- US Department of Health and Human Services. NCHS Data Brief. No. 351. October 2019. Available at: https://www.cdc.gov/nchs/data/databriefs/ db351-h.pdf. Accessed January 21, 2021.
- Centers for Disease Control and Prevention. National vital statistics reports,
- births: final data for 2018, November 29, 2019, volume 69, number 13. Available at: https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_13-508. pdf. Accessed January 21, 2021.
- American Society for Reproductive Medicine. ASRM press release/bulletin, March 26, 2020: More than 74 thousand babies born from assisted reproductive technology cycles done in 2018. Available at: https://www.cdc.gov/ nchs/data/databriefs/db351-h.pdf. Accessed January 21, 2021.
- Reynolds MA, Schieve LA, Martin JA, Jeng G, Macaluso M. Trends in multiple births conceived using assisted reproductive technology, United States, 1997–2000. Pediatrics 2003;111(5 Part 2):1159–62.
- Adashi EY, Barri PN, Berkowitz R, Braude P, Bryan E, Carr J, et al. Infertility therapy-associated multiple pregnancies (births): an ongoing epidemic. Reprod Biomed Online 2003;7:515–42.
- Dickey RP. The relative contribution of assisted reproductive technologies and ovulation induction to multiple births in the United States 5 years after the Society for Assisted Reproductive Technology/American Society for Reproductive Medicine recommendation to limit the number of embryos transferred. Fertil Steril 2007;88:1554–61.
- White C, Wyshak G. Inheritance in human dizygotic twinning. N Engl J Med 1964;271:1003–5.
- Centers for Disease Control and Prevention (CDC). Contribution of assisted reproductive technology and ovulation-inducing drugs to triplet and higher-order multiple births—US, 1980–1997. MMWR Morb Mortal Wkly Rep 2000;49:535–8.
- MacGillivray I. Epidemiology of twin pregnancy. Semin Perinatol 1986;10: 4–8.
- Norwitz ER. Multiple pregnancy: trends past, present, and future. Infertil Reprod Med Clin North Am 1998;9:351–69.
- Kiely JL, Kleinman JC, Kiely M. Triplets and higher-order multiple births. Time trends and infant mortality. Am J Dis Child 1992;146:862–8.
- Bulmer MC. The biology of twinning. London: Oxford University Press; 1970.
- Abusheikha N, Salha O, Sharma V, Brinsden P. Monozygotic twinning and IVF/ICSI treatment: a report of 11 cases and review of literature. Hum Reprod Update 2000;6:396–403.
- Toledo MG. Is there increased monozygotic twinning after assisted reproductive technology? Aust N Z J Obstet Gynaecol 2005;45:360–4.
- Tur R, Barri PN, Coroleu B, Buxaderas R, Parera N, Balasch J. Use of a prediction model for high-order multiple implantation after ovarian stimulation with gonadotropins. Fertil Steril 2005;83:116–21.
- Templeton A, Morris JK. Reducing the risk of multiple births by transfer of two embryos after in vitro fertilization. N Engl J Med 1998;339:573–7.
- Jain T, Missmer SA, Hornstein MD. Trends in embryo-transfer practice and in outcomes of the use of assisted reproductive technology in the United States. N Engl J Med 2004;350:1639–45.
- Saito H, Tsutsumi O, Noda Y, Ibuki Y, Hiroi M. Do assisted reproductive technologies have effects on the demography of monozygotic twinning? Fertil Steril 2000;74:178–9.
- Alikani M, Noyes N, Cohen J, Rosenwaks Z. Monozygotic twinning in the human is associated with the zona pellucida architecture. Hum Reprod 1994;9:1318–21.
- Kanter JR, Boulet SL, Kawwass JF, Jamieson DJ, Kissin DM. Trends and correlates of monozygotic twinning after single embryo transfer. Obstet Gynecol 2015;125:111–7.
- Busnelli A, Dallagiovanna C, Reschini M, Paffoni A, Fedele L, Somigliana E. Risk factors for monozygotic twinning after in vitro fertilization: a systematic review and meta-analysis. Fertil Steril 2019;111:302–17.
- Moayeri SE, Behr B, Lathi RB, Westphal LM, Milki AA. Risk of monozygotic twinning with blastocyst transfer decreases over time: an 8-year experience. Fertil Steril 2007;87:1028–32.
- Ombelet W, de Sutter P, van der Elst J, Martens G. Multiple gestation and infertility treatment: registration, reflection and reaction—the Belgian project. Hum Reprod Update 2005;11:3–14.
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Munson ML. Births: final data for 2002. Natl Vital Stat Rep 2003;52:1–113.
- Henderson CE, Scarpelli S, LaRosa D, Divon MY. Assessing the risk of gestational diabetes in twin gestation. J Natl Med Assoc 1995;87:757–8.
- Wein P, Warwick MM, Beischer NA. Gestational diabetes in twin pregnancy: prevalence and long-term implications. Aust N Z J Obstet Gynaecol 1992;32:325–7.
- Adams DM, Sholl JS, Haney EI, Russell TL, Silver RK. Perinatal outcome associated with outpatient management of triplet pregnancy. Am J Obstet Gynecol 1998;178:843–7.
- Martin JA, MacDorman MF, Mathews TJ. Triplet births: trends and outcomes, 1971–94. Vital Health Stat 1997;21:1–20.
- March of Dimes Birth Defects Foundation (a joint document of the March of Dimes, the American College of Obstetricians and Gynecologists, and the American Society for Reproductive Medicine). Multiple pregnancy and birth: considering fertility treatments. September 2006. Available at: https://www.marchofdimes.org/materials/multiple-pregnancy-and-birth-considering-fertility-treatments.pdf. Accessed January 2, 2021.
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Obstetrics, Society for Maternal-Fetal Medicine, ACOG Joint Editorial Committee. ACOG practice bulletin no. 56: multiple gestation: complicated twin, triplet, and high-order multifetal pregnancy. Obstet Gynecol 2004;104:869–83.
- Seoud MA, Toner JP, Kruithoff C, Muasher SJ. Outcome of twin, triplet, and quadruplet in vitro fertilization pregnancies: the Norfolk experience. Fertil Steril 1992;57:825–34. Albrecht JL, Tomich PG. The maternal and neonatal outcome of triplet gestations. Am J Obstet Gynecol 1996;174:1551–6.
- Kauppila A, Jouppila P, Koivisto M, Moilanen I, Ylikorkala O. Twin pregnancy. A clinical study of 335 cases. Acta Obstet Gynecol Scand 1975; 44:5–12.
- D'Alton ME, Mercer BM. Antepartum management of twin gestation: ultrasound. Clin Obstet Gynecol 1990;33:42-51.Evans MI, Britt DW. Fetal reduction. Semin Perinatol 2005;29:321–329.
- Torok O, Lapinski R, Salafia CM, Bernasko J, Berkowitz RL. Multifetal pregnancy reduction is not associated with an increased risk of intrauterine growth restriction, except for very-high-order multiples. Am J Obstet Gynecol 1998;179:221–5.
- Evans MI, Britt DW. Fetal reduction. Semin Perinatol 2005;29:321–9.
- Tummers P, De Sutter P, Dhont M. Risk of spontaneous abortion in singleton and twin pregnancies after IVF/ICSI. Hum Reprod 2003;18: 1720–3.
- Landy HJ, Keith LG. The vanishing twin: a review. Hum Reprod Update 1998;4:177–83.
- Corson SL, Dickey RP, Gocial B, Batzer FR, Eisenberg E, Huppert L, et al. Outcome in 242 in vitro fertilization-embryo replacement or gamete intrafallopian transfer-induced pregnancies. Fertil Steril 1989;51:644–50.
- Landy HJ, Weiner S, Corson SL, Batzer FR, Bolognese RJ. The ‘‘vanishing twin’’: ultrasonographic assessment of fetal disappearance in the first trimester. Am J Obstet Gynecol 1986;155:14–9.
- de Sutter P, Delbaere I, Gerris J, Verstraelen H, Goetgeluk S, van der Elst J, et al. Birthweight of singletons after assisted reproduction is higher after single- than after double-embryo transfer. Hum Reprod 2006;21:2633–7.
- Pinborg A, Lidegaard O, la Cour Freiesleben N, Andersen AN. Consequences of vanishing twins in IVF/ICSI pregnancies. Hum Reprod 2005; 20:2821–9.
- Pinborg A, Lidegaard O, Freiesleben NL, Andersen AN. Vanishing twins: a predictor of small-for-gestational age in IVF singletons. Hum Reprod 2007; 22:2707–14.
- Anand D, Platt MJ, Pharoah PO. Vanishing twin: a possible cause of cerebral impairment. Twin Res Hum Genet 2007;10:202–9.
- Dudley DK, d’Alton ME. Single fetal death in twin gestation. Semin Perinatol 1986;10:65–72.
- Strong TH JR, Brar HS. Placenta previa in twin gestations. J Reprod Med 1989;34:415–6.
- Benirschke K. The biology of the twinning process: how placentation influences outcome. Semin Perinatol 1995;19:342–50.
- Collins J. Cost efficiency of reducing multiple births. Reprod Biomed Online 2007;15(Suppl 3):35–9.
- Lemos EV, Zhang D, Van Voorhis BJ, Hu XH. Healthcare expenses associated with multiple vs singleton pregnancies in the United States. Am J Obstet Gynecol 2013 December;209:586.e1–11.
- van Heesch MM, Evers JL, van der Hoeven MA, Dumoulin JC, van Beijsterveldt CE, Bonsel GJ, et al. Hospital costs during the first 5 years of life for multiples compared with singletons born after IVF or ICSI. Hum Reprod 2015;30:1481–90.
- US Department of Agriculture. Expenditures on children by families, Available at: https://fns-prod.azureedge.net/sites/default/files/crc2015_ March2017.pdf. Accessed January 22, 2021.
- Practice Committee of the American Society for Reproductive Medicine and the Practice Committee for the Society for Assisted Reproductive Technologies. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertil Steril 2021;116:651–4.
- Martin JA, Hamilton BE, Ventura SJ, Osterman MJ, Kirmeyer S, Mathews TJ, et al. Births: final data for 2009. Natl Vital Stat Rep 2011;60:1–70.
- Hamilton BH, McManus B. The effects of insurance mandates on choices and outcomes in infertility treatment markets. Health Econ 2012;21: 994–1016.
- Jain T, Harlow BL, Hornstein MD. Insurance coverage and outcomes of in vitro fertilization. N Engl J Med 2002;347:661–6.
- Practice Committee, Society for Assisted Reproductive Technology and the American Society for Reproductive Medicine. Guidelines on the number of embryos transferred. Fertil Steril 2004;82:773–4.
- Practice Committee of the Society for Assisted Reproductive Technology; Practice Committee of the American Society for Reproductive Medicine. Guidelines on number of embryos transferred. Fertil Steril 2006;86(Suppl 1):S51–2.
- Practice Committee of Society for Assisted Reproductive Technology; Practice Committee of American Society for Reproductive Medicine. Guidelines on number of embryos transferred. Fertil Steril 2008;90(Suppl): S163–4.
- Practice Committee of the American Society for Reproductive Medicine and the Practice Committee of the Society for Assisted Reproductive Technology. Criteria for number of embryos to transfer: a committee opinion. Fertil Steril 2013;99:44–6.
- Practice Committee of the American Society for Reproductive Medicine. Practice Committee of the Society for Assisted Reproductive Technology. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertil Steril 2017;107:901–3.
- Mancuso AC, Boulet SL, Duran E, Munch E, Kissin DM, Van Voorhis BJ. Elective single embryo transfer in women less than age 38 years reduces multiple birth rates, but not live birth rates, in United States fertility clinics. Fertil Steril 2016;106:1107–14.
- Stern JE, Cedars MI, Jain T, Klein NA, Beaird CM, Grainger DA, et al. Assisted reproductive technology practice patterns and the impact of embryo transfer guidelines in the US. Fertil Steril 2007;88:275–82.
- Centers for Disease Control and Prevention. Annual ART success rates reports. Available at: https://www.cdc.gov/art/reports/archive.html. Accessed January 21, 2021.
- Society for Assisted Reproductive Technology. More single embryo transfers. Available at:https://www.sart.org/globalassets/sart/infographics/ more-single-embryo-transfers.png. Accessed December 10, 2021.
- Society for Assisted Reproductive Technology. Fewer multiple pregnancies. Available at: https://www.sart.org/globalassets/sart/infographics/fewer-multiple-pregnancies.png. Accessed December 10, 2021.
- Ethics Committee of the American Society for Reproductive Medicine. Cross-border reproductive care: an Ethics Committee opinion. Fertil Steril 2016;106:1627–33.
- Perkins KM, Boulet SL, Jamieson DJ, Kissin DM. National Assisted Reproductive Technology Surveillance System (NASS) Group. Trends and outcomes of gestational surrogacy in the United States. Fertil Steril 2016; 106:435–42.e2.
- Kulkarni AD, Jamieson DJ, Jones HW JR, Kissin DM, Gallo MF, Macaluso M, et al. Fertility treatments and multiple births in the United States. N Engl J Med 2013;369:2218–25.
- Makhijani RB, Coulter M, Thorne J, Bartels C, Nulsen J, Engmann L, et al. Impact of preimplantation genetic testing for aneuploidy (PGT-A) on gestational carrier (GC) cycles in the United States. Fertil Steril 2019;112:e227.
- Kamath MS, Mascarenhas M, Kirubakaran R, Bhattacharya S. Number of embryos for transfer following in vitro fertilisation or intra-cytoplasmic sperm injection. Cochrane Database Syst Rev 2020;8:CD003416.
- Kuwayama M, Vajta G, Kato O, Leibo SP. Highly efficient vitrification method for cryopreservation of human oocytes. Reprod Biomed Online 2005;11:300–8.
- Gerris J, de Sutter P. Elective single embryo transfer. In: Carrell DT, Schlegel P, van Voorhis B, Racowsky C, editors. Biennial review of reproduction. Totawa (NJ): Humana; 2008:171–83.
- Gardner DK, Surrey E, Minjarez D, Leitz A, Stevens J, Schoolcraft WB. Single blastocyst transfer: a prospective randomized trial. Fertil Steril 2004;81: 551–5.
- McLernon DJ, Harrild K, Bergh C, Davies MJ, de Neubourg D, Dumoulin JC, et al. Clinical effectiveness of elective single versus double embryo transfer: meta-analysis of individual patient data from randomised trials. BMJ 2010; 341:c6945.
- Thurin A, Hausken J, Hillensjo T, Jablonowska B, Pinborg A, Strandell A, et al. Elective single-embryo transfer versus double-embryo transfer in in vitro fertilization. N Engl J Med 2004;351:2392–402.
- Styer AK, Wright DL, Wolkovich AM, Veiga C, Toth TL. Single-blastocyst transfer decreases twin gestation without affecting pregnancy outcome. Fertil Steril 2008;89:1702–8.
- Criniti A, Thyer A, Chow G, Lin P, Klein N, Soules M. Elective single blastocyst transfer reduces twin rates without compromising pregnancy rates. Fertil Steril 2005;84:1613–9.
- Ryan GL, Sparks AE, Sipe CS, Syrop CH, Dokras A, van Voorhis BJ. A mandatory single blastocyst transfer policy with educational campaign in a United States IVF program reduces multiple gestation rates without sacrificing pregnancy rates. Fertil Steril 2007;88:354–60.
- Csokmay JM, Hill MJ, Chason RJ, Hennessy S, James AN, Cohen J, et al. Experience with a patient-friendly, mandatory, single-blastocyst transfer policy: the power of one. Fertil Steril 2011;96:580–4.
- Papanikolaou EG, Camus M, Kolibianakis EM, van Landuyt L, van Steirteghem A, Devroey P. In vitro fertilization with single blastocyst-stage versus single cleavage-stage embryos. N Engl J Med 2006;354: 1139–46.
- Rivera RM, Stein P, Weaver JR, Mager J, Schultz RM, Bartolomei MS. Manipulations of mouse embryos prior to implantation result in aberrant expression of imprinted genes on day 9.5 of development. Hum Mol Genet 2008;17:1–14.
- Practice Committee of Society for Assisted Reproductive Technology; Practice Committee of American Society for Reproductive Medicine. Elective single-embryo transfer. Fertil Steril 2012;97:835–42.
- Forman EJ, Tao X, Ferry KM, Taylor D, Treff NR, Scott RT Jr. Single embryo transfer with comprehensive chromosome screening results in improved ongoing pregnancy rates and decreased miscarriage rates. Hum Reprod 2012;27:1217–22.
- Forman EJ, Hong KH, Ferry KM, Tao X, Taylor D, Levy B, et al. In vitro fertilization with single euploid blastocyst transfer: a randomized controlled trial. Fertil Steril 2013;100:100–7.e1.
- Forman EJ, Hong KH, Franasiak JM, Scott RT JR. Obstetrical and neonatal outcomes from the BEST Trial: single embryo transfer with aneuploidy screening improves outcomes after in vitro fertilization without compromising delivery rates. Am J Obstet Gynecol 2014;210: 157.e1–6.
- Munn,e S, Kaplan B, Frattarelli JL, Child T, Nakhuda G, Shamma FN, et al. Preimplantation genetic testing for aneuploidy versus morphology as selection criteria for single frozen-thawed embryo transfer in good-prognosis patients: a multicenter randomized clinical trial. Fertil Steril 2019;112: 1071–9.e7.
- Franik S, Eltrop SM, Kremer JA, Kiesel L, Farquhar C. Aromatase inhibitors (letrozole) for subfertile women with polycystic ovary syndrome. Cochrane Database Syst Rev 2018;5:CD010287.
- Wang R, Kim BV, van Wely M, Johnson NP, Costello MF, Zhang H, et al. Treatment strategies for women with WHO group II anovulation: systematic review and network meta-analysis. BMJ 2017;356:j138.
- Practice Committees of the American Society for Reproductive Medicine and Society for Reproductive Endocrinology and Infertility. Use of exogenous gonadotropins for ovulation induction in anovulatory women: a committee opinion. Fertil Steril 2020;113:66–70.
- Zolton JR, Lindner PG, Terry N, DeCherney AH, Hill MJ. Gonadotropins versus oral ovarian stimulation agents for unexplained infertility: a systematic review and meta-analysis. Fertil Steril 2020;113:417–25.e1.
- Danhof NA, Wang R, van Wely M, van der Veen F, Mol BWJ, Mochtar MH. IUI for unexplained infertility-a network meta-analysis. Hum Reprod Update 2020;26:1–15.
- Reindollar RH, Regan MM, Neumann PJ, Levine BS, Thornton KL, Alper MM, et al. A randomized clinical trial to evaluate optimal treatment for unexplained infertility: the fast track and standard treatment (FASTT) trial. Fertil Steril 2010;94:888–99.
- Goldman MB, Thornton KL, Ryley D, Alper MM, Fung JL, Hornstein MD, et al. A randomized clinical trial to determine optimal infertility treatment in older couples: the Forty and Over Treatment Trial (FORT-T). Fertil Steril 2014;101:1574–81.e1-2.
- Carpinello OJ, Jahandideh S, Yamasaki M, Hill MJ, Decherney AH, Stentz N, et al. Does ovarian stimulation benefit ovulatory women undergoing therapeutic donor insemination? Fertil Steril 2021;115:638–45.
- Diamond MP, Legro RS, Coutifaris C, Alvero R, Robinson RD, Casson P, et al. Letrozole, gonadotropin, or clomiphene for unexplained infertility. N Engl J Med 2015;373:1230–40.
- Ragni G, Maggioni P, Guermandi E, Testa A, Baroni E, Colombo M, et al. Efficacy of double intrauterine insemination in controlled ovarian hyperstimulation cycles. Fertil Steril 1999;72:619–22.
- Danhof NA, van Wely M, Repping S, Koks C, Verhoeve HR, de Bruin JP, et al. Follicle stimulating hormone versus clomiphene citrate in intrauterine insemination for unexplained subfertility: a randomized controlled trial. Hum Reprod 2018;33:1866–74.
- Rosen MP, Shen S, Dobson AT, Rinaudo PF, McCulloch CE, Cedars MI. A quantitative assessment of follicle size on oocyte developmental competence. Fertil Steril 2008;90:684–90.
- Evans MB, Stentz NC, Richter KS, Schexnayder B, Connell M, Healy MW, et al. Mature follicle count and multiple gestation risk based on patient age in intrauterine insemination cycles with ovarian stimulation. Obstet Gynecol 2020;135:1005–14.
- Danhof NA, van Wely M, Repping S, van der Ham DP, Klijn N, Janssen ICAH, et al. Gonadotrophins or clomiphene citrate in couples with unexplained infertility undergoing intrauterine insemination: a cost-effectiveness analysis. Reprod Biomed Online 2020;40:99–104.
- Albano C, Platteau P, Nogueira D, Cortvrindt R, Smitz J, Devroey P. Avoidance of multiple pregnancies after ovulation induction by supernumerary preovulatory follicular reduction. Fertil Steril 2001;76:820–2.
- de Geyter C, de Geyter M, Castro E, Bals-Pratsch M,Nieschlag E, Schneider HP. Experience with transvaginal ultrasound-guided aspiration of supernumerary follicles for the prevention of multiple pregnancies after ovulation induction and intrauterine insemination. Fertil Steril 1996;65:1163–8.
- de Geyter C, de Geyter M, Nieschlag E. Low multiple pregnancy rates and reduced frequency of cancellation after ovulation induction with gonadotropins, if eventual supernumerary follicles are aspirated to prevent polyovulation. J Assist Reprod Genet 1998;15:111–6.
- Ghesquiere SL, Castelain EG, Spiessens C, Meuleman CL, d’Hooghe TM. Relationship between follicle number and (multiple) live birth rate after controlled ovarian hyperstimulation and intrauterine insemination. Am J Obstet Gynecol 2007;197:589.e1–5.
- Evans MI, Britt DW. Fetal reduction in 2008. Curr Opin Obstet Gynecol 2008;20:386–93.
- Evans MI, Britt DW. Multifetal pregnancy reduction: evolution of the ethical arguments. Semin Reprod Med 2010;28:295–302.
- American College of Obstetricians and Gynecologists. Committee on Ethics. ACOG committee opinion. No. 369. June 2007. Multifetal pregnancy reduction. Obstet Gynecol 2007;109:1511–5.
- Wimalasundera RC. Selective reduction and termination of multiple pregnancies. Semin Fetal Neonatal Med 2010;15:327–35.
- Evans MI, Berkowitz RL, Wapner RJ, Carpenter RJ, Goldberg JD, Ayoub MA, et al. Improvement in outcomes of multifetal pregnancy reduction with increased experience. Am J Obstet Gynecol 2001;184:97–103.
- Chescheir NC. Outcomes of multifetal pregnancy reductions. Clin Obstet Gynecol 2004;47:134–45.
- Papageorghiou AT, Avgidou K, Bakoulas V, Sebire NJ, Nicolaides KH. Risks of miscarriage and early preterm birth in trichorionic triplet pregnancies with embryo reduction versus expectant management: new data and systematic review. Hum Reprod 2006;21:1912–7.
- Zipori Y, Haas J, Berger H, Barzilay E. Multifetal pregnancy reduction of triplets to twins compared with non-reduced triplets: a meta-analysis. Reprod Biomed Online 2017;35:296–304.
- Stone J, Belogolovkin V, Matho A, Berkowitz RL, Moshier E, Eddleman K. Evolving trends in 2000 cases of multifetal pregnancy reduction: a single center experience. Am J Obstet Gynecol 2007;197:394.e1–4.
- Skiadas CC, Missmer SA, Benson CB, Acker D, Racowsky C. Impact of selective reduction of the monochorionic pair in in vitro fertilization triplet pregnancies on gestational length. Fertil Steril 2010;94:2930–1.
- Zaner RM, Boehm FH, Hill GA. Selective termination in multiple pregnancies: ethical considerations. Fertil Steril 1990;54:203–5.
- Garel M, Stark C, Blondel B, Lefebvre G, Vauthier-Brouzes D, Zorn JR. Psychological reactions after multifetal pregnancy reduction: a 2-year follow-up study. Hum Reprod 1997;12:617–22.
- Schreiner-Engel P, Walther VN, Mindes J, Lynch L, Berkowitz RL. First-trimester multifetal pregnancy reduction: acute and persistent psychologic reactions. Am J Obstet Gynecol 1995;172(2 Pt 1):541–7.
- Munks EB, Edelman AB, Jensen JT, Nichols MD, Burry K, Patton P. IVF patients’ attitudes toward multifetal pregnancy reduction. J Reprod Med 2007;52:635–8.
- Dodd JM, Crowther CA. Reduction of the number of fetuses for women with triplet and higher order multiple pregnancies. Cochrane Database Syst Rev 2003;2:CD003932.
Practice Documents
ASRM Practice Documents have been developed to assist physicians with clinical decisions regarding the care of their patients.
Tobacco or marijuana use and infertility: a committee opinion (2023)
In the United States, approximately 21% of adults report some form of tobacco use, although 18% report marijuana use.
Prevention of moderate and severe ovarian hyperstimulation syndrome: a guideline (2023)
Ovarian hyperstimulation syndrome is a serious complication associatedwith assisted reproductive technology.
Definition of infertility: a committee opinion (2023)
‘‘Infertility’’ is a disease, condition, or status characterized by several factors.
Clinical management of mosaic results from preimplantation genetic testing for aneuploidy of blastocysts: a committee opinion (2023)
This document incorporates studies about mosaic embryo transfer and provides evidence-based considerations for embryos with mosaic results on PGT-A.More Resources

ASRM MAC Tool 2021
The ASRM Müllerian Anomaly Classification 2021 (MAC2021) includes cervical and vaginal anomalies and standardize terminology within an interactive tool format.

EMR Shared Phrases/Template Library
This resource includes phrases shared by ASRM physician members to provide a template for individuals to create their own EMR phrases.
ASRM Practice Documents

ASRM Ethics Opinions
Ethics Committee Reports are drafted by the members of the ASRM Ethics Committee on the tough ethical dilemmas of reproductive medicine.

Coding Corner Q & A
The Coding Corner Q & A is a list of previously submitted and answered questions from ASRM members about coding. Answers are available to ASRM Members only.

COVID-19 Resources
A compendium of ASRM resources concerning the Novel Corona virus (SARS-COV-2) and COVID-19.

Patient Resources
ReproductiveFacts.org provides a wide range of information related to reproductive health and infertility through patient education fact sheets, infographics, videos, and other resources.